Anatomy and Physiology of the Coronary Arteries
Related Subjects:
| AP of the Coronary Arteries
|Atherosclerosis
|Ischaemic heart disease
|Acute Coronary Syndrome (ACS): Complications
|Acute Coronary Syndrome (ACS)
The coronary circulation supplies oxygen and nutrients to the myocardium and is uniquely adapted to meet high metabolic demand. Impairment of coronary blood flow rapidly leads to myocardial ischaemia, arrhythmia, and infarction. Understanding coronary anatomy and flow dynamics is essential for interpreting ECG changes, managing acute coronary syndromes, and guiding revascularisation.
❤️ Left Coronary Artery (LCA)🫀
- Origin: Arises from the left aortic sinus of the ascending aorta.
- Main Branches:
- 🌟 Left Anterior Descending (LAD) – Supplies anterior septum and apex; proximal occlusion = “widowmaker”.
- ↪️ Left Circumflex (LCx) – Courses in AV groove; gives obtuse marginal branches.
- Supplied Territories:
- LAD: Anterior LV wall, anterior 2/3 of septum, apex.
- LCx: Lateral LV wall ± posterior wall (in left dominance).
💙 Right Coronary Artery (RCA)
- Origin: Arises from the right aortic sinus.
- Main Branches:
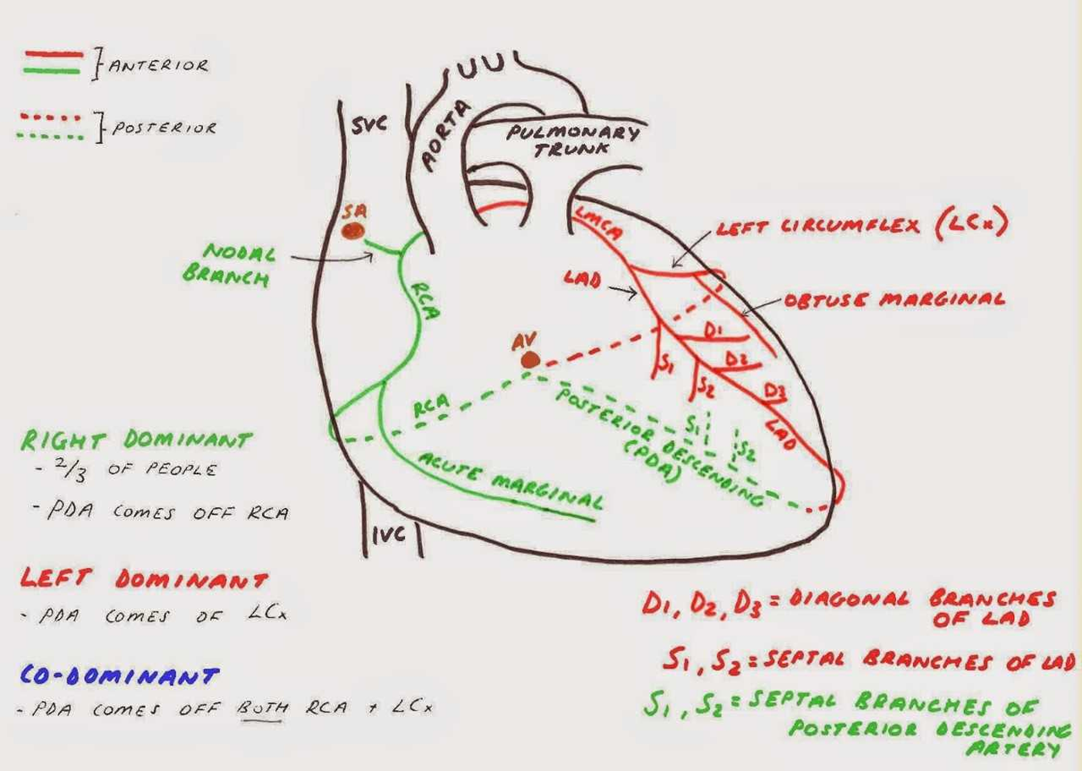
- Posterior Descending Artery (PDA): From RCA in ~85% (right dominance).
- Right Marginal Artery: Supplies RV free wall.
- Supplied Territories:
- RCA: Right atrium, RV, SA node (~60%), AV node (~80%).
- PDA: Inferior LV wall, posterior septum.
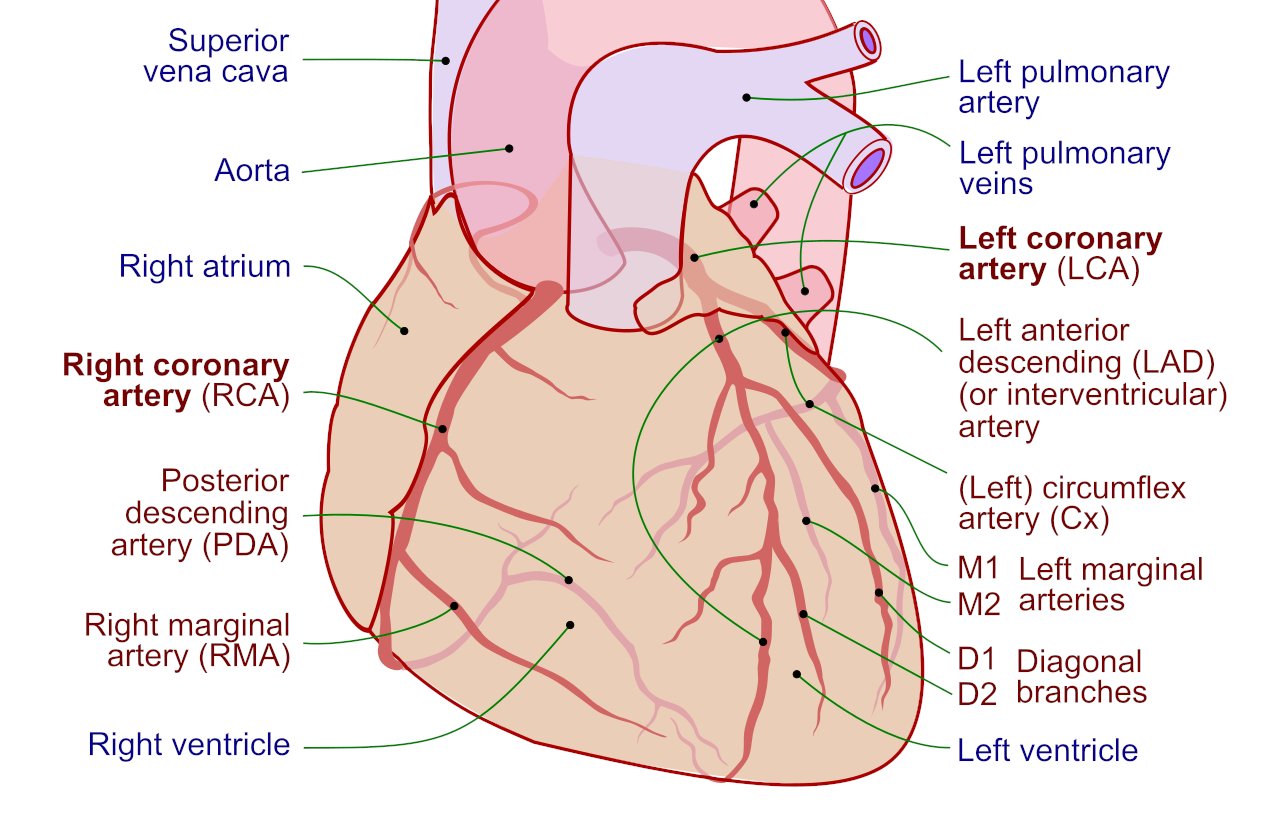
🫀 Coronary Artery Anatomy
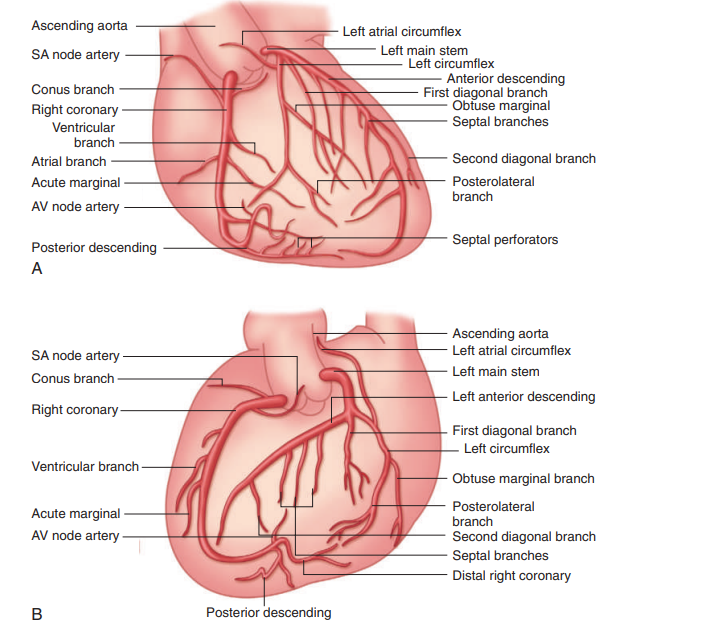
📊 Major Coronary Arteries - Summary
| Artery |
Origin |
Branches |
Supplied Areas |
| LCA |
Left aortic sinus |
LAD, LCx |
Most of LV myocardium |
| RCA |
Right aortic sinus |
PDA, Right marginal |
RA, RV, inferior LV, conduction system |
| PDA |
RCA (85%) / LCx (8–10%) |
- |
Posterior LV + septum |
| LMCA |
Left aortic sinus |
LAD + LCx |
Large LV territory |
📉 Coronary Occlusion and ECG Changes
| Artery |
ECG Leads |
Typical Changes |
Territory |
| LAD |
V1–V4 |
ST elevation, Q waves |
Anterior/septal LV |
| LCx |
I, aVL, V5–V6 |
Lateral ST elevation |
Lateral LV |
| RCA |
II, III, aVF |
Inferior ST elevation |
Inferior LV/RV |
| PDA |
V7–V9 |
Posterior ST elevation |
Posterior LV |
| LMCA |
Widespread |
Global ST changes |
Large LV area |
💡 Coronary Blood Flow
Unlike most organs, coronary perfusion occurs predominantly during diastole. During systole, myocardial contraction compresses intramyocardial vessels, particularly in the left ventricle, reducing flow. Tachycardia shortens diastole and therefore reduces coronary perfusion.
⚙️ Coronary Flow Dynamics
- ⏱️ Diastolic dominance: Maximal perfusion in ventricular relaxation.
- 🔄 Autoregulation: Maintains stable flow across MAP 60–140 mmHg.
- 💪 Metabolic coupling: Flow rises in proportion to oxygen demand.
- 🫀 Subendocardial vulnerability: Inner myocardium is most susceptible to ischaemia.
🧬 Regulation of Coronary Tone
- Local metabolites: Adenosine, CO₂, H⁺, K⁺ → vasodilation.
- Endothelial factors: Nitric oxide (NO), prostacyclin.
- Neurohumoral: Sympathetic tone modulates flow indirectly via demand.
- Structural disease: Atherosclerosis reduces vasodilatory reserve.
🚫 Vasoconstrictors
- Endothelin-1, Angiotensin II, Thromboxane A2
- α-adrenergic stimulation (noradrenaline)
- Serotonin (5-HT)
✅ Vasodilators
- Nitric oxide (NO), Prostacyclin (PGI₂)
- Adenosine, Bradykinin
- β₂-agonists
- Calcium-channel blockers
- Nitrates (clinical use)
🩺 Clinical Integration
Coronary artery disease impairs vasodilatory reserve, meaning flow cannot increase adequately during stress. This results in exertional angina, ECG changes, and myocardial stunning. In acute plaque rupture, abrupt occlusion causes transmural infarction, electrical instability, and cardiogenic shock if untreated.
- Reduced diastolic time (tachycardia, AF) worsens ischaemia.
- Hypotension reduces coronary perfusion pressure.
- LV hypertrophy increases oxygen demand.
- Anaemia reduces oxygen delivery.
✅ Makindo Exam & Clinical Pearls
- LAD occlusion = highest mortality (large LV territory).
- Inferior MI + hypotension → suspect RV infarction (RCA).
- Tachycardia worsens angina by reducing diastolic filling.
- Subendocardium is always first to become ischaemic.
- Left main disease causes global ECG changes and shock.
