
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Developmental Dislocation (Dysplasia) of the Hip (DDH)
Related Subjects: | Developmental Dysplasia of the Hip (DDH) | Slipped Upper Femoral Epiphysis (SUFE) | Perthes Disease (Osteochondritis of the Hip)
👶 Babies swaddled tightly with hips/knees straight have a much higher risk of DDH. ⏰ Early detection is critical → late diagnosis often means major surgery, poorer outcomes, and long-term disability.
📖 About
- Occurs in ~1–2 per 1,000 babies needing treatment.
- A spectrum: from mild acetabular dysplasia → subluxation → frank dislocation.
- Ball (femoral head) is unstable in socket (acetabulum) → may dislocate.
⚙️ Aetiology
- Hip is a ball-and-socket joint but is malformed in DDH.
- Femoral head may be loose, subluxed, or fully dislocated.
- Multifactorial: mechanical (breech), genetic, intrauterine factors.
📌 Risk Factors
- 👧 Female sex, 🍼 first-born child.
- 🤰 Breech delivery (all breech girls need hip USS).
- 👨👩👧 Family history (parents/siblings).
- 💧 Oligohydramnios (reduced amniotic fluid).
🗂️ Classification
- Dislocated: femoral head completely outside socket.
- Dislocatable: head in acetabulum but easily displaced on exam.
- Subluxatable: femoral head loose, moves within socket but not fully dislocated.
🔍 Key neonatal tests: - Ortolani’s test (reduce dislocated hip). - Barlow’s test (provoke dislocation).
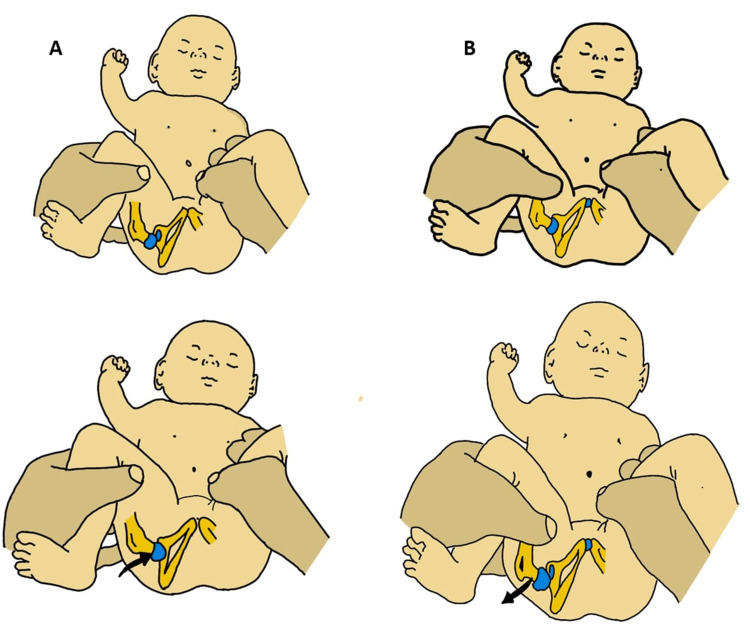
🩺 Clinical Signs (<3 months)
- Asymmetrical skin folds (inguinal, gluteal, thigh).
- Klisic line: from greater trochanter to ASIS → should pass through umbilicus; falls below if DDH.
- Ortolani & Barlow positive → USS indicated.
- USS preferred <6 months (femoral head cartilaginous). X-ray useful >6 months.
🔍 Clinical Presentation
- Routine hip screen: birth + 6–8 weeks.
- Unequal leg length, asymmetric movement, limited abduction.
- Older infants: limp, toe-walking, waddling gait.
🧪 Investigations
- Ultrasound (USS): gold standard <6 months. Detects subtle instability.
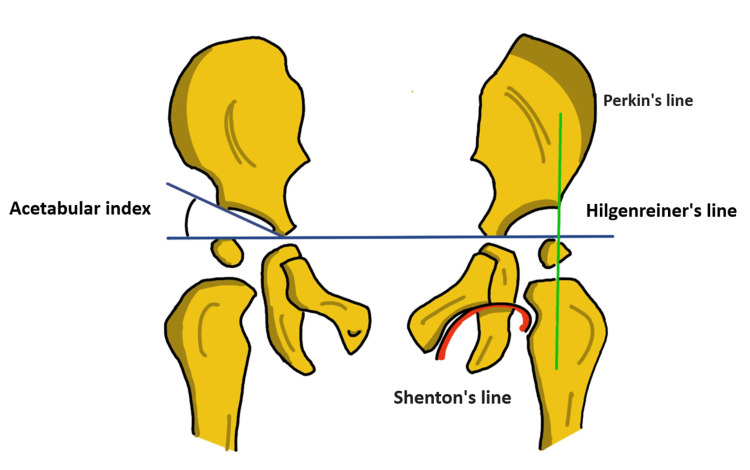
- X-ray (>6 months): - Hilgenreiner’s line (through triradiate cartilages). - Perkins line (perpendicular from acetabular edge). - Shenton’s line (should be continuous curve). - Acetabular index: normally 27.5° at birth → 20° by age 2;>30° abnormal.
🚨 Complications
- Untreated → early hip OA, chronic pain, gait disturbance.
- Leg length difference, persistent limp, “duck-like” gait.
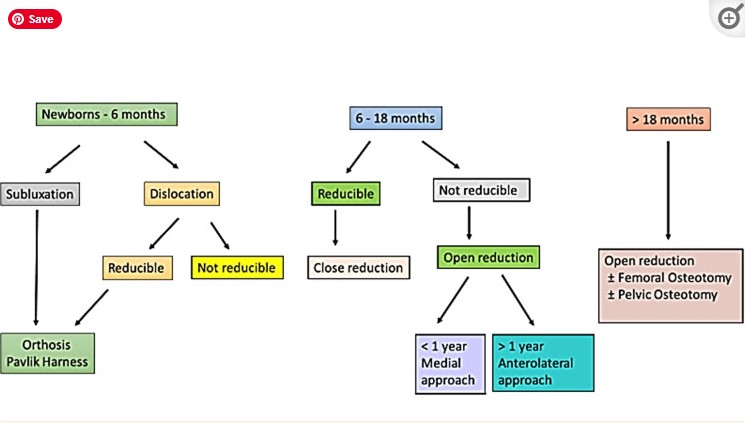
🩹 Management
- 0–6 months: Pavlik harness or brace (keeps femoral head in socket).
- 6–12 months: Harness or brace, sometimes spica casting after reduction.
- 12–24 months: Closed reduction + spica cast. Skin traction sometimes pre-reduction. If fails → open reduction + spica cast.
- >2 years / severe cases: Often require open surgery ± pelvic/femoral osteotomies.
- Even after treatment → socket may remain shallow, may need later corrective surgery.
💡 Teaching Pearls
- Always check hip abduction in newborns. Limited abduction is a red flag. - Breech girls always get a hip USS regardless of exam findings. - Late presentation = much harder to treat and worse outcomes. - “Pavlik harness saves hips” – but only if used early!
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery