
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Radial Ulnar and Median Palsy of the Hand
Radial, ulnar, and median nerve palsies are common exam and clinical presentations. They are best understood by linking anatomy → muscle imbalance → characteristic posture. In practice, pattern recognition at the bedside often localises the lesion before imaging or nerve studies.
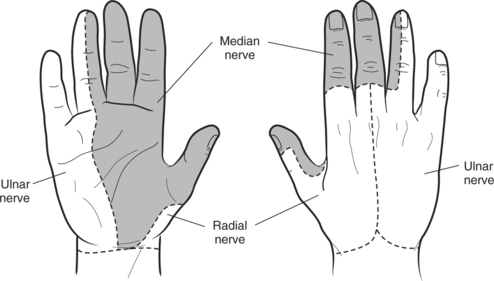
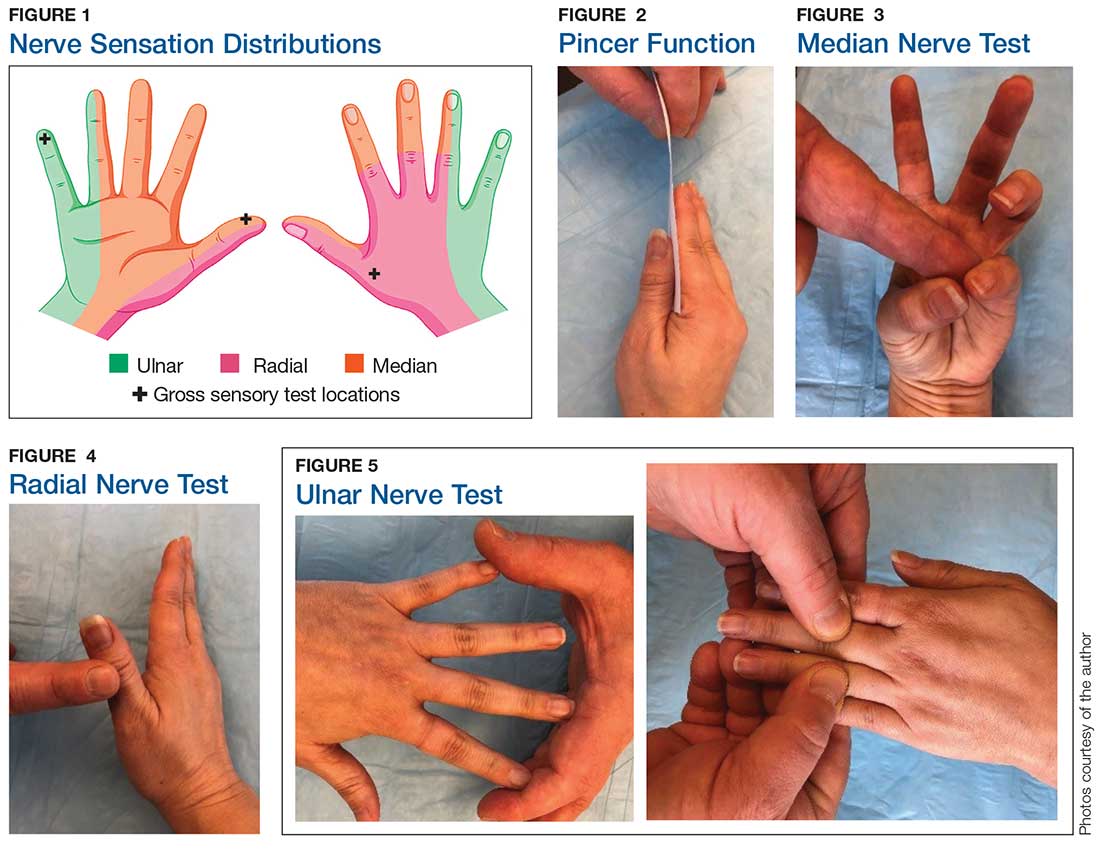
Sensation
🟦 Radial Nerve Palsy
The radial nerve supplies the extensor compartment of the arm and forearm. Injury leads to unopposed flexor activity, resulting in loss of wrist and finger extension. Common mechanisms include humeral shaft fractures and prolonged compression (“Saturday night palsy”).
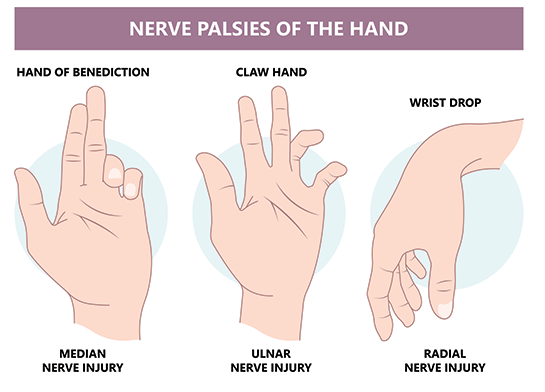
- Motor: Wrist drop, inability to extend fingers and thumb
- Sensory: Dorsal first web space
- Key sign: Wrist remains flexed when patient attempts extension
🟩 Ulnar Nerve Palsy
The ulnar nerve innervates most intrinsic hand muscles, critical for fine motor control. Loss of interossei causes finger abduction/adduction failure and a characteristic imbalance between long flexors and extensors. Lesions are common at the elbow (cubital tunnel) or wrist (Guyon’s canal).
- Motor: Weak finger abduction/adduction, weak grip
- Posture: Clawing of ring and little finger (worse distally)
- Sensory: Little finger + ulnar half of ring finger
🟥 Median Nerve Palsy
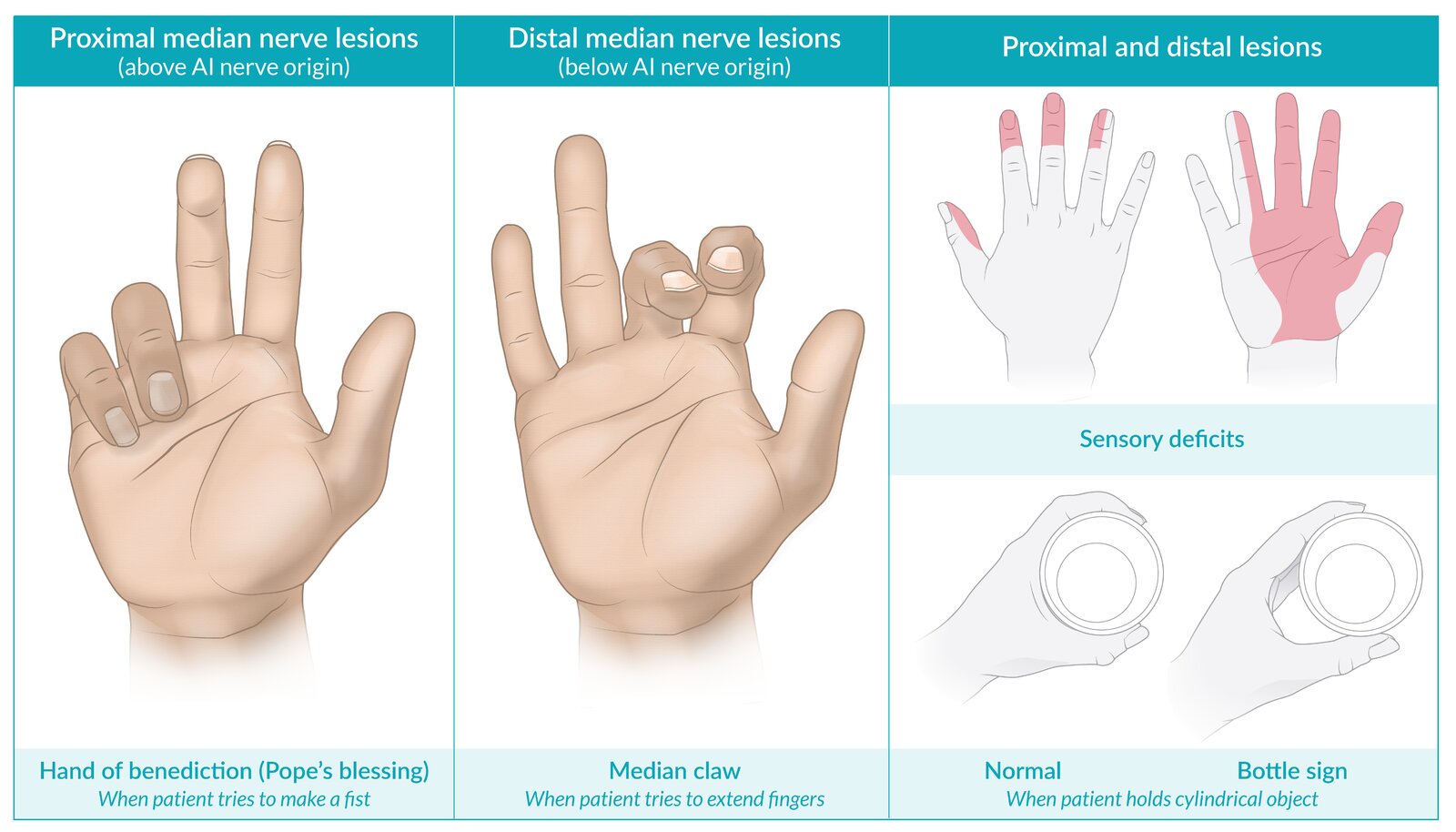
The median nerve supplies most forearm flexors and thenar muscles. In proximal lesions, loss of finger flexion becomes apparent when the patient attempts to make a fist. Distal lesions primarily affect thumb opposition and precision grip.
- Motor: Weak wrist flexion, loss of thumb opposition
- Posture: “Hand of benediction” on making a fist
- Sensory: Palmar thumb, index, middle, and half ring finger
🧪 Bedside Localisation Tips
Ask the patient to extend the wrist (radial), abduct/adduct fingers (ulnar), and oppose the thumb (median). Always compare both sides and consider proximal causes (cervical radiculopathy) if findings are mixed. In UK practice, document neurovascular status carefully after trauma and before/after splinting.
🔑 Clinical Pearl
Radial = extension, Ulnar = intrinsic hand control, Median = precision grip. If you can picture the muscle imbalance, the diagnosis usually becomes obvious at the bedside.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery