
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Central Pontine Myelinolysis (Osmotic Demyelination Syndrome) ✅
⚠️ Osmotic demyelination syndrome (ODS) is a feared complication of over-rapid correction of chronic hyponatraemia. 🎯 The clinician must balance the danger of ongoing severe hyponatraemia (seizures, cerebral oedema, coma) against the risk of raising sodium too quickly. 🚨 Patients at particularly high risk of ODS include those with alcohol dependence, malnutrition, advanced liver disease, hypokalaemia, and very low or prolonged hyponatraemia.
🧠 Osmotic Demyelination Syndrome (formerly “Central Pontine Myelinolysis”)
- ODS refers to non-inflammatory demyelination caused by osmotic injury, classically affecting the central pons but also sometimes the basal ganglia, thalamus, cerebellum, and other extrapontine sites.
- Central pontine myelinolysis (CPM) is therefore one anatomical subtype of the broader syndrome.
- It is most strongly associated with over-rapid correction of chronic hyponatraemia, although it can occasionally occur in other major osmotic shifts.
- The syndrome is often delayed: neurological deterioration may occur 2–6 days after sodium correction, which can create a false sense of security early on.
📖 Why the brain is vulnerable
In chronic hyponatraemia, brain cells adapt by extruding osmoles to reduce cerebral swelling. This adaptation protects against cerebral oedema, but it also makes the brain biochemically fragile. If serum sodium then rises too quickly, extracellular osmolality increases before brain cells can readapt, so water is pulled out of cells, leading to cellular dehydration, oligodendrocyte injury, and demyelination. The pons is classically affected because of its dense mixture of fibre tracts and unique metabolic vulnerability, but extrapontine structures may also be involved.
⚠️ Aetiology
- Most important cause: overly rapid correction of chronic hypotonic hyponatraemia.
- Iatrogenic risk: hypertonic saline, uncontrolled water diuresis, recovery from SIADH, adrenal replacement, or correction of hypovolaemia can all produce unexpectedly rapid sodium rises.
- Other osmotic settings: severe shifts in serum osmolality, including marked hypernatraemia or major osmotic disturbance after transplantation or critical illness.
- Classic associated states: alcohol dependence, malnutrition, cirrhosis, liver transplantation, hypokalaemia, and profound chronic hyponatraemia.
📌 High-Risk Groups
- 🍺 Alcohol dependence
- 🍽️ Severe malnutrition / cachexia
- 🫀 Advanced liver disease or post–liver transplant state
- ⚡ Hypokalaemia (important and often under-recognised)
- 🧪 Very low starting sodium, especially <120 mmol/L and particularly if prolonged
- ⏳ Chronic hyponatraemia lasting more than 48 hours or of uncertain duration
🚫 Unsafe Rates of Correction
- Avoid increases >10 mmol/L in the first 24 hours.
- Avoid increases >8 mmol/L per 24 hours thereafter.
- In high-risk patients, many experts aim for ≤8 mmol/L in 24 hours from the outset.
- Remember: overcorrection can occur even without further treatment, for example when a patient suddenly begins to excrete large volumes of dilute urine.
🩺 Clinical Features
- Timing: often a delayed neurological decline after initial biochemical improvement.
- Early features: confusion, behavioural change, lethargy, dysarthria.
- Brainstem signs: dysarthria, dysphagia, pseudobulbar symptoms, ophthalmoplegia.
- Motor deficits: spastic quadriparesis or quadriplegia.
- Consciousness: reduced consciousness, akinetic mutism, or coma in severe cases.
- Severe end-stage pattern: a locked-in–like syndrome may occur if pontine damage is extensive.
- Extrapontine disease: may produce parkinsonism, dystonia, catatonia, or other movement disorders.
🧠 Classic Clinical Pattern
A common exam pattern is this: a patient with severe chronic hyponatraemia initially appears to improve as the sodium rises, then after a delay develops dysarthria, dysphagia, spastic weakness, and reduced consciousness. That biphasic story is highly suggestive of ODS. The syndrome can mimic stroke, encephalitis, or metabolic encephalopathy, which is why careful review of the recent sodium trend is so important.
🔍 Differential Diagnosis
- 🧠 Brainstem stroke
- 🦠 Brainstem encephalitis (for example Listeria rhombencephalitis)
- ⚡ Non-convulsive status epilepticus or post-ictal state
- 💊 Sedative or toxic drug effect
- 🫁 Hypoxic-ischaemic injury
- 🦴 Wernicke’s encephalopathy or other nutritional/toxic-metabolic syndromes
🧪 Investigations
- Serial U&Es: the most important investigation is often the sodium trajectory over time rather than a single sodium value.
- Check potassium, magnesium, phosphate, glucose, renal function, and liver profile.
- FBC, inflammatory markers, and blood cultures if sepsis or encephalitis is a competing diagnosis.
- MRI brain is the imaging test of choice, but may be normal early.
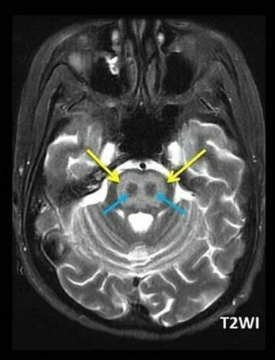
- MRI findings: T2/FLAIR hyperintensity in the central pons, sometimes described as a trident or bat-wing pattern; extrapontine lesions may also be present.
- CSF is usually non-specific and mainly helps exclude alternative diagnoses.
- EEG may be needed if reduced consciousness could reflect seizure activity.
📸 Imaging Pearl
Do not exclude ODS just because the first MRI is normal. Radiological changes may lag behind clinical deterioration, so a repeat MRI may be needed if suspicion remains high. In practice, the diagnosis is often made from the combination of risk factors, recent sodium overcorrection, and a characteristic delayed neurological syndrome.
💊 Management
- Prevention is the key treatment ✅.
- Correct chronic hyponatraemia cautiously, using frequent sodium checks and careful reassessment.
- Monitor serum sodium every 2–4 hours during active correction in severe cases.
- Monitor urine output closely: sudden high urine output may herald rapid aquaresis and overcorrection.
- Replace potassium carefully, because potassium repletion itself can increase serum sodium.
- If sodium is rising too fast: stop hypertonic therapy and seek senior/specialist advice urgently.
- Relowering therapy may be considered in specialist practice, typically with desmopressin and/or hypotonic fluid such as 5% dextrose, to re-slow or reverse overcorrection.
- If ODS is established: treatment is mainly supportive ABC, ITU if needed for airway protection, nutrition, VTE prevention, neurorehabilitation, speech and swallow input, and management of complications.
🛑 Practical Prevention Rules
- Always ask: is this acute hyponatraemia or chronic / unknown duration?
- Patients with severe symptoms may need hypertonic saline, but even then the sodium rise must be controlled.
- Do not chase a “normal sodium” quickly - the initial goal is usually to make the patient safer, not to normalise the number immediately.
- In high-risk groups, be even more conservative and discuss early with renal/endocrine/critical care teams depending on local pathways.
📉 Prognosis
- Mild cases: partial or substantial recovery may occur, especially with rehabilitation.
- Moderate to severe cases: persistent bulbar dysfunction, spasticity, cognitive impairment, or severe disability may remain.
- Severe pontine injury: may result in a locked-in–like state or death.
- The best prognostic intervention is still prevention by controlled sodium correction.
🎓 Teaching Pearls
- ODS is usually caused by treatment, not by the low sodium itself.
- Chronic hyponatraemia is dangerous to correct too fast; acute hyponatraemia is dangerous not to correct fast enough.
- Hypokalaemia increases ODS risk and should always raise your level of caution.
- A delayed deterioration after apparent improvement is a classic clue.
- “Central pontine myelinolysis” is only part of the picture; extrapontine demyelination is common enough that ODS is the better term.
📚 References
- NICE CKS: Hyponatraemia
- Society for Endocrinology (2022): Emergency management of severe and moderately severely symptomatic hyponatraemia in adult patients
- European Society of Endocrinology / European guideline on hypotonic hyponatraemia
- Martin RJ. Central Pontine and Extrapontine Myelinolysis. JNNP.
- Verbalis JG et al. Treatment Guidelines for Hyponatremia.
🖼️ Trident / Piglet Signs
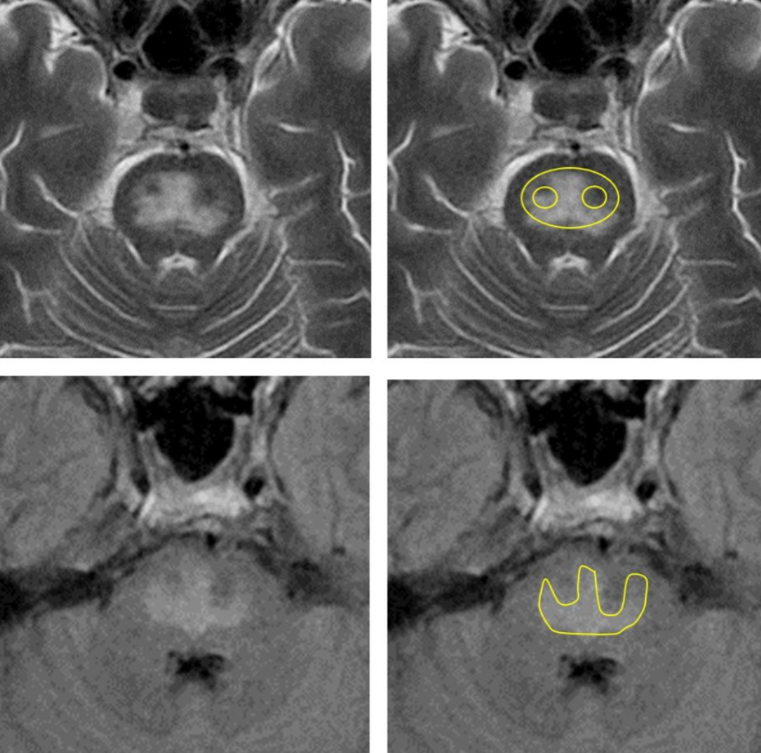
🖼️ Piglet Sign
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery