
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Intravenous fluids ✅
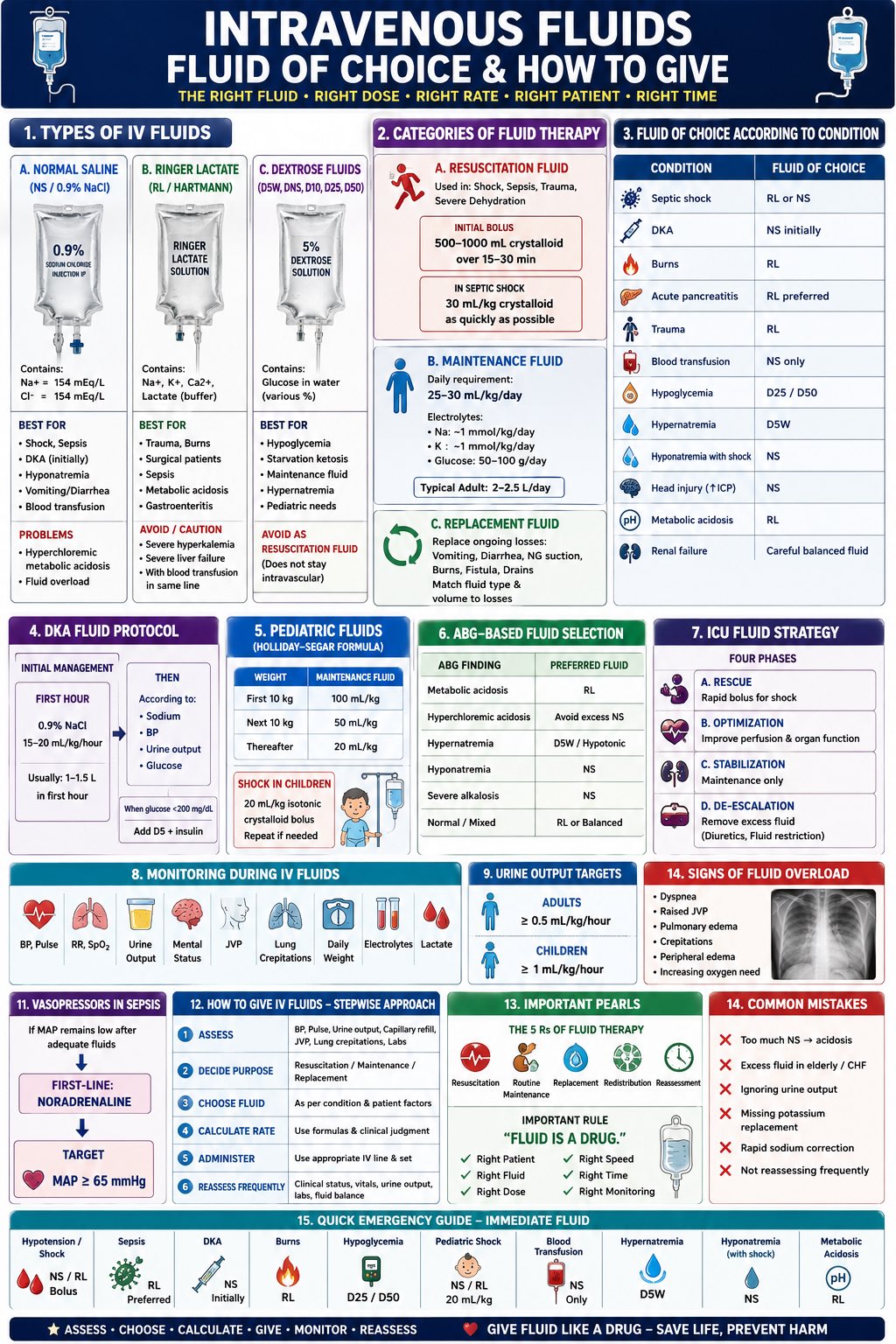
💧 Intravenous (IV) fluid therapy is used when a patient cannot meet their fluid or electrolyte needs orally or enterally. NICE CG174 advises that IV fluids should be prescribed using the 5 Rs: Resuscitation, Routine maintenance, Replacement, Redistribution and Reassessment. IV fluids should be stopped as soon as oral or enteral intake is adequate.
IV Fluids 💧
IV fluids are medicines and should be prescribed with the same care as antibiotics or anticoagulants. The aim is to restore or maintain intravascular volume, correct deficits, replace ongoing losses and avoid harm from under-resuscitation or fluid overload.
The 5 Rs 🧠
- Resuscitation: urgent fluid bolus for hypovolaemia or shock.
- Routine maintenance: daily water and electrolyte needs when oral intake is inadequate.
- Replacement: replacing losses such as vomiting, diarrhoea, drains or stoma output.
- Redistribution: fluid shifts in sepsis, burns, pancreatitis, oedema or hypoalbuminaemia.
- Reassessment: review response, fluid balance, electrolytes and clinical status regularly.
Initial assessment 🔍
- Check airway, breathing and circulation if acutely unwell.
- Assess pulse, blood pressure, capillary refill, JVP and mucous membranes.
- Look for pulmonary oedema, peripheral oedema and postural hypotension.
- Review NEWS, urine output, fluid balance chart and daily weight if available.
- Check U&Es, creatinine, glucose and relevant blood gases or lactate.
- Review comorbidities: heart failure, renal disease, liver disease, frailty and malnutrition.
Signs IV fluid resuscitation may be needed 🚨
- Systolic blood pressure less than 100 mmHg.
- Heart rate more than 90 beats per minute.
- Capillary refill time more than 2 seconds or cold peripheries.
- Respiratory rate more than 20 breaths per minute.
- NEWS of 5 or more.
- Passive leg raise suggests fluid responsiveness.
- Raised lactate or clinical features of shock.
Fluid types table 🧪
| Fluid | Common use | Important cautions |
|---|---|---|
| 0.9% sodium chloride
“normal saline” |
Resuscitation, replacement of sodium/chloride-rich losses, some drug infusions. | High chloride load may cause hyperchloraemic metabolic acidosis. Monitor chloride if large volumes are used. |
| Balanced crystalloid
e.g. Hartmann’s, Plasma-Lyte |
Often used for resuscitation and perioperative replacement. | Contains electrolytes closer to plasma. Use caution in severe hyperkalaemia depending on local policy. |
| Glucose 5% | Free water replacement once glucose is metabolised; sometimes used in hypernatraemia under careful supervision. | Not suitable for resuscitation. Can cause hyponatraemia if used inappropriately. |
| Sodium chloride 0.18% with glucose 4% | Often used as part of routine maintenance regimens. | May cause hyponatraemia if over-prescribed. Usually needs potassium added via pre-prepared bags if indicated. |
| Fluids with potassium | Maintenance or replacement when potassium is needed. | Check renal function and potassium first. Do not add potassium manually to bags unless trained/local policy permits. |
| Human albumin solution 4–5% | Selected cases such as severe sepsis where specialist input supports use. | Not routine first-line fluid. Use according to senior/specialist advice. |
Resuscitation fluids 🚑
For fluid resuscitation, NICE recommends a crystalloid containing sodium in the range of 130–154 mmol/L, giving a 500 mL bolus over less than 15 minutes, then reassessing. This is not “set and forget”: reassess after each bolus for improvement or fluid overload.
- Use ABCDE assessment.
- Give a 500 mL crystalloid bolus if hypovolaemic.
- Reassess pulse, BP, capillary refill, respiratory rate, oxygenation and urine output.
- Stop or slow fluids if breathlessness, crackles, raised JVP or pulmonary oedema develops.
- Seek senior help early if repeated boluses are needed.
Routine maintenance 🧃
Routine maintenance is for patients who cannot drink enough but are not shocked and do not have major ongoing losses. NICE suggests initial daily requirements of 25–30 mL/kg/day water, about 1 mmol/kg/day sodium, potassium and chloride, and 50–100 g/day glucose to limit starvation ketosis.
- Use ideal body weight in obesity.
- Most patients rarely need more than 3 litres per day for maintenance alone.
- Prescribe less, for example 20–25 mL/kg/day, in older, frail, renal impairment, cardiac failure or malnourished patients.
- Maintenance fluids do not provide nutrition.
- Review oral intake daily and stop IV fluids as soon as possible.
Replacement and redistribution 🔄
Replacement fluids are used when there are existing deficits or ongoing abnormal losses. Redistribution occurs when fluid is in the wrong compartment, such as oedema, sepsis, pancreatitis or post-operative fluid shifts.
- Measure losses from vomiting, diarrhoea, drains, NG tubes, stomas and urine.
- Replace like with like where possible.
- Check sodium, potassium, chloride, urea and creatinine trends.
- Seek senior help for severe sepsis, renal failure, heart failure, liver disease, major oedema, hyponatraemia or hypernatraemia.
Monitoring 📊
- Review fluid status at least daily if continuing IV fluids.
- Check U&Es and creatinine daily initially.
- Use fluid balance charts accurately.
- Measure weight twice weekly, or more often if clinically indicated.
- Monitor urine output, especially in acutely unwell patients.
- Monitor chloride if giving large volumes of 0.9% sodium chloride.
Common harms ⚠️
- Fluid overload: breathlessness, crackles, raised JVP, oedema, pulmonary oedema.
- Hypovolaemia: hypotension, tachycardia, poor perfusion, AKI, low urine output.
- Hyponatraemia: confusion, seizures, reduced consciousness.
- Hypernatraemia: thirst, agitation, confusion, neurological complications.
- Hyperkalaemia: weakness, arrhythmias, ECG changes.
- Hyperchloraemic acidosis: can follow large volumes of 0.9% sodium chloride.
Patients needing extra caution 🧓
- Older or frail patients.
- Heart failure.
- Chronic kidney disease or acute kidney injury.
- Liver disease or ascites.
- Sepsis or shock.
- Post-operative patients.
- Malnourished patients or those at risk of refeeding syndrome.
- Patients with severe electrolyte disturbance.
Common exam and ward pitfalls ❌
- Prescribing “one bag stat” without a clear indication.
- Using maintenance fluids for resuscitation.
- Using glucose 5% for shock.
- Forgetting potassium requirements in maintenance fluids.
- Giving too much fluid to frail patients or those with heart failure.
- Ignoring oral intake, drug diluents, blood products and enteral feeds.
- Not checking U&Es after starting IV fluids.
- Continuing IV fluids after the patient is drinking adequately.
Makindo exam summary 🎯
For exams, think: Why does this patient need IV fluid? If shocked, give a crystalloid bolus and reassess. If simply not drinking, prescribe maintenance based on weight and risk factors. If losing fluid, replace the measured loss. Always review electrolytes, renal function, fluid balance and signs of overload.
References 📚
- NICE. Intravenous fluid therapy in adults in hospital. Clinical guideline CG174. Published 10 December 2013. Last updated 5 May 2017.
- NICE CG174 recommends prescribing IV fluids using the 5 Rs: resuscitation, routine maintenance, replacement, redistribution and reassessment.
- NICE CG174 recommends routine maintenance of 25–30 mL/kg/day water, approximately 1 mmol/kg/day sodium, potassium and chloride, and 50–100 g/day glucose.
- NICE CG174 recommends a 500 mL crystalloid bolus over less than 15 minutes for IV fluid resuscitation, followed by reassessment.
Disclaimer 📚
This article is for medical education and revision only. IV fluid prescribing should follow NICE CG174, local Trust policy, senior clinical advice and patient-specific factors including renal function, cardiac function, electrolyte results, fluid balance, sepsis status and perioperative context.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Education
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Paediatrics
- Palliative
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery