
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Rectum
|Anatomy of the Ear |AP of the Oesophagus |AP of the Diaphragm |AP of the Large Bowel (Colon, Rectum, Anal Canal) |AP of Small Bowel |AP of the Biliary system |AP of the Bone Marrow |Anatomy of the Eye |AP of the Pharynx |AP of the Larynx |AP of the Nose |AP of Male Genitalia |AP of the Breast |AP of the Stomach |AP of the Rectum |Anatomy of the SpleenThe rectum is the final segment of the large bowel, specialised for temporary stool storage and coordinated defecation while maintaining continence. Its function depends on rectal compliance (ability to stretch), sensory signalling of filling, autonomic reflexes (internal sphincter), voluntary control (external sphincter + pelvic floor), and the anorectal angle.
1) Gross Anatomy
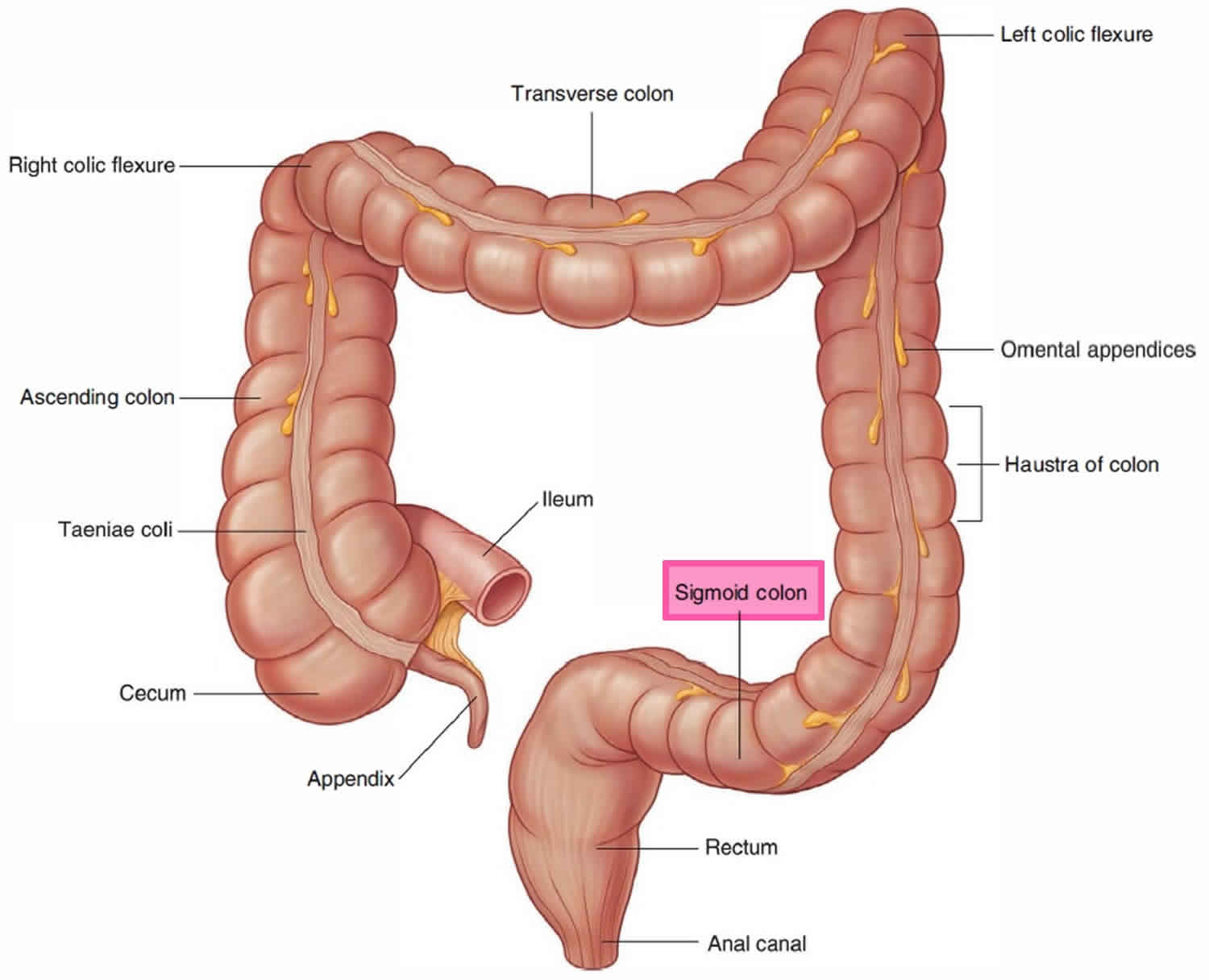
- Length & extent: approximately 12–15 cm, extending from the sigmoid colon (at the rectosigmoid junction) to the anal canal.
- Location: in the pelvis, lying anterior to the sacrum and coccyx.
- Curvatures:
- Anteroposterior flexures: follow sacral curve and perineal alignment.
- Lateral flexures correspond to the internal rectal folds (valves of Houston), helping support stool and possibly aiding continence.
- Peritoneal relations: upper rectum is partly covered by peritoneum; lower rectum is mostly extraperitoneal (important for spread of disease and surgical planning).
2) Key Internal Features
- Rectal ampulla: distal dilated rectum acting as a storage reservoir.
- Valves of Houston: transverse mucosal folds that can help support the fecal column and slow premature descent.
- Anorectal junction: transition into anal canal; closely linked to continence mechanisms.
3) Rectal Wall Histology (Layers)
The rectum is lined by columnar epithelium like the colon and contains goblet cells for lubrication. At the anal canal there is a key epithelial transition to stratified squamous epithelium, reflecting the shift from absorption/storage to abrasion-resistant passage.
- Mucosa: simple columnar epithelium with abundant goblet cells → mucus lubrication.
- Submucosa: vessels, lymphatics, and the submucosal nerve plexus.
- Muscularis propria: inner circular and outer longitudinal smooth muscle.
– Unlike the colon, the longitudinal layer becomes more continuous (taeniae coli spread out). - Adventitia/Serosa: connective tissue outer layer; serosal covering depends on level.
4) Blood Supply and Venous Drainage 🩸
Rectal blood supply has a “three-tier” pattern that mirrors its embryological and pelvic relationships. Venous drainage is clinically important because it forms part of the portosystemic anastomosis at the anorectal region.
- Arterial supply:
- Superior rectal artery (terminal branch of inferior mesenteric artery) → main supply to upper rectum.
- Middle rectal arteries (from internal iliac) → variable contribution to mid/lower rectum.
- Inferior rectal arteries (from internal pudendal) → anal canal and distal region.
- Venous drainage:
- Superior rectal vein → inferior mesenteric vein → portal system.
- Middle and inferior rectal veins → internal iliac system → systemic circulation.
- Clinical: this junction explains the anorectal portosystemic connection relevant to haemorrhoidal disease and portal hypertension (though haemorrhoids are not simply “rectal varices”).
5) Lymphatic Drainage (High-yield for Malignancy)
- Upper rectum: along superior rectal vessels → inferior mesenteric nodes.
- Lower rectum: to internal iliac nodes.
- Anal canal: lymphatic drainage depends on level (below pectinate line tends toward superficial inguinal nodes).
6) Innervation 🧠
Rectal function is coordinated by the enteric nervous system plus autonomic input, while continence relies heavily on intact sacral pathways and the somatic pudendal nerve to the external sphincter.
- Parasympathetic: pelvic splanchnic nerves (S2–S4) → increase rectal motility and mediate the rectoanal inhibitory reflex.
- Sympathetic: lumbar splanchnics via hypogastric plexus → reduce motility, increase internal sphincter tone.
- Somatic: pudendal nerve (S2–S4) → external anal sphincter and pelvic floor voluntary control; also conveys sensation from distal anal canal.
7) Physiology
🧺 A) Storage and Compliance
- Reservoir function: the rectum (especially the ampulla) stores stool until socially appropriate defecation.
- Compliance: rectal walls distend with relatively small rises in pressure, allowing storage without constant urgency.
- Sensation: stretch receptors detect filling and discriminate gas vs liquid vs solid, helping continence decisions.
🚪 B) Continence Mechanisms
Continence is maintained by a layered system: (1) internal anal sphincter tone (autonomic), (2) external sphincter and pelvic floor (voluntary), (3) the anorectal angle created by puborectalis, and (4) rectal compliance and sensation.
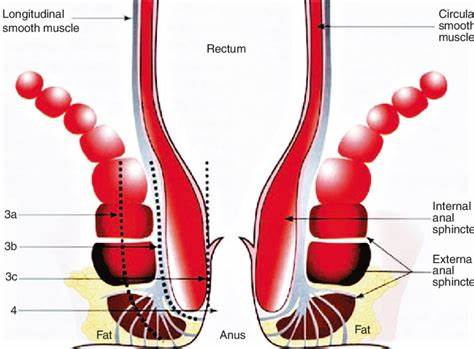
- Internal anal sphincter (IAS): smooth muscle; provides most resting tone; involuntary.
- External anal sphincter (EAS): skeletal muscle; voluntary squeeze and reflex contraction.
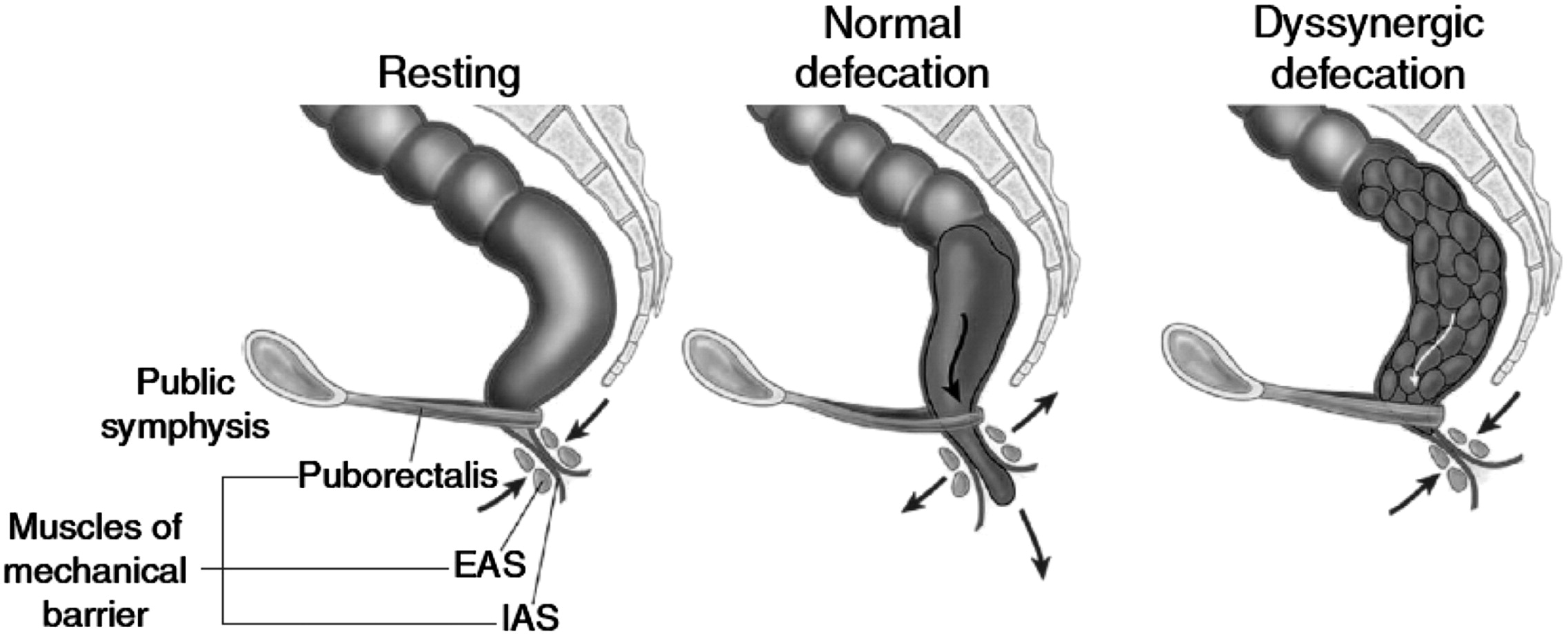
- Puborectalis (pelvic floor): sling around anorectal junction; maintains the anorectal angle (a key continence “kink”).
- Anal cushions: vascular submucosal pads contribute to fine sealing; enlargement can contribute to symptomatic haemorrhoids.
🔁 C) The Defecation Reflex (Step-by-step)
Defecation begins with rectal distension, triggering an involuntary reflex relaxation of the internal sphincter (RAIR). Voluntary control then determines whether defecation proceeds (external sphincter relaxation + pelvic floor descent) or is postponed (external sphincter contraction + rectal accommodation).
- 1. Rectal filling: mass movements from colon push stool into rectum → distension.
- 2. RAIR (rectoanal inhibitory reflex): distension → parasympathetic/enteric reflex → IAS relaxes.
- 3. Sampling reflex: brief IAS relaxation allows contents to contact sensory mucosa → discrimination of gas vs stool.
- 4a. If defecation is deferred: EAS contracts; puborectalis tightens; rectum may accommodate and urgency reduces.
- 4b. If defecation proceeds: EAS relaxes; puborectalis relaxes → anorectal angle straightens; rectal contraction + abdominal wall/Valsalva increases intra-abdominal pressure → expulsion.
💧 D) Absorption and Secretion
- Absorption: limited compared with colon, but some water and electrolytes can be absorbed.
- Mucus secretion: goblet cells lubricate stool passage and protect mucosa.
8) Common Rectal Disorders (Clinical Correlation)
- Haemorrhoids: symptomatic enlargement/displacement of anal cushions → bleeding, prolapse, discomfort.
- Anal fissure: tear causing severe pain and bleeding; often linked to constipation and hypertonic sphincter.
- Rectal prolapse: full-thickness protrusion; associated with pelvic floor weakness and chronic straining.
- Proctitis: inflammation (IBD, infection, radiation) → urgency, bleeding, tenesmus.
- Rectal cancer: anatomy and lymphatics guide staging and surgery; symptoms can include bleeding, altered bowel habit, tenesmus.
- Fecal incontinence: can result from sphincter injury (obstetric/iatrogenic), neuropathy, reduced rectal compliance, or severe diarrhoea.
9) Diagnosis and Treatment (Overview)
- Assessment:
- History: bleeding, pain, tenesmus, change in bowel habit, incontinence, weight loss.
- DRE: assesses tone, masses, tenderness, stool characteristics.
- Proctoscopy/sigmoidoscopy: direct visualisation of distal bowel.
- Colonoscopy: evaluates full colon when indicated (e.g., bleeding, anaemia, cancer concerns).
- Imaging: pelvic MRI for rectal cancer staging; CT for systemic staging; defecography for prolapse/functional disorders when needed.
- Management principles:
- Constipation-driven symptoms: fibre, hydration, osmotic laxatives, toileting posture, avoid straining.
- Haemorrhoids/fissures: stool softening + topical therapy; procedural options when refractory.
- Proctitis: treat underlying cause (IBD therapy, antimicrobials, radiation strategies).
- Pelvic floor dysfunction: pelvic floor physiotherapy/biofeedback.
- Neoplasia: MDT-led care (endoscopic/surgical/oncology pathways).
✅ Summary
The rectum is a specialised storage and control organ where continence depends on rectal compliance, sensory signalling, the internal anal sphincter (autonomic tone and RAIR), and the external sphincter + pelvic floor (voluntary control and anorectal angle). Understanding its vascular, lymphatic, and neural anatomy is essential for interpreting bleeding patterns, staging malignancy, and managing common conditions like haemorrhoids, fissures, prolapse, and proctitis.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery