
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Focal Segmental Glomerulosclerosis (FSGS)
Related Subjects: |Metabolic acidosis |Lactic acidosis |Acute Kidney Injury (AKI) / Acute Renal Failure |Renal/Kidney Physiology |Chronic Kidney Disease (CKD) |Anaemia in Chronic Kidney Disease |Analgesic Nephropathy |Medullary Sponge kidney |IgA Nephropathy (Berger's disease) |HIV associated nephropathy (HIVAN) |Balkan endemic nephropathy (BEN) |Adult Polycystic kidney disease |Focal Segmental Glomerulosclerosis (FSGS)
🧪 Focal Segmental Glomerulosclerosis (FSGS) is a major cause of nephrotic syndrome and chronic kidney disease worldwide. "Focal" → only some glomeruli are affected. "Segmental" → only part of each affected glomerulus shows sclerosis.
📘 About
- One of the most common causes of end-stage renal disease (ESRD) globally.
- Presents with proteinuria - nephrotic (>3.5 g/day) or sub-nephrotic.
- Incidence is rising, with a significant public health burden.
🧬 Aetiology & Pathophysiology
- Podocyte injury and depletion are the central mechanism → impaired filtration barrier → proteinuria.
- Likely immune-mediated: possible circulating plasma factor (explains recurrence post-transplant & steroid responsiveness).
- Genetic forms seen especially in children and young adults (e.g., podocin or nephrin mutations).
- Shares features with Minimal Change Disease (MCD) but biopsy reveals segmental sclerosis.
🔍 Microscopy (Biopsy)
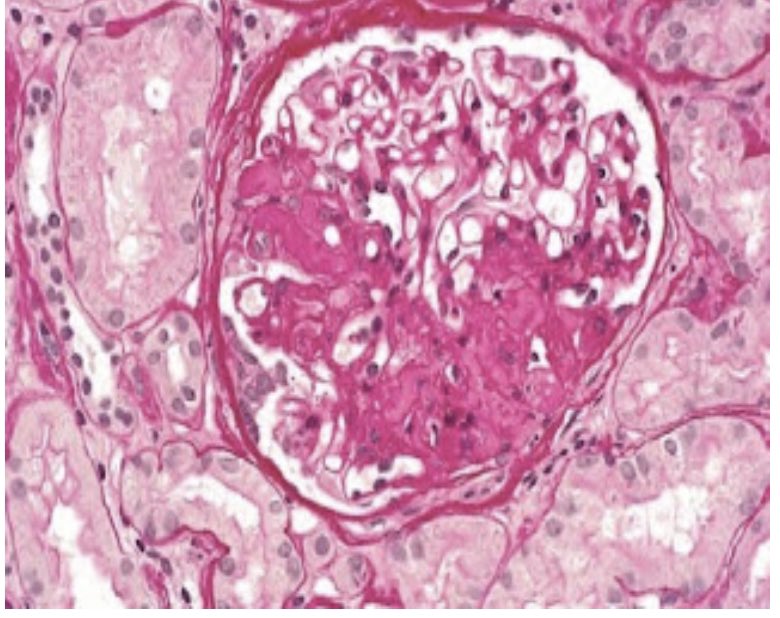
🎯 Renal biopsy: segmental sclerosis, hyalinosis, and podocyte effacement (on EM). Immunofluorescence may show IgM and C3 deposits.
📎 Associations
- 🏥 Nephropathies: reflux nephropathy, analgesic nephropathy.
- 🦠 Infections: HIV, malaria.
- 💉 Substances: IV heroin use.
- 🧬 Haemoglobinopathies: sickle cell disease.
- ⚖️ Other: severe obesity, adaptive response to reduced nephron mass.
- 🔄 Post-transplant recurrence: occurs in up to 30% of patients, often leading to graft loss.
👩⚕️ Clinical Presentation
- Nephrotic syndrome: oedema, frothy urine, hypoalbuminaemia, hyperlipidaemia.
- Hypertension is common (especially adults).
- Microscopic haematuria in some cases.
- Prothrombotic tendency → ↑ risk of DVT, PE, or renal vein thrombosis.
🔬 Investigations
- Dipstick: proteinuria ± blood.
- 24h urine protein: quantifies nephrotic-range proteinuria.
- U&Es: rising creatinine → renal impairment.
- USS: kidneys usually normal size/echogenicity.
- Biopsy (gold standard): focal & segmental sclerosis of glomerular tufts, mesangial expansion.
💊 Management
- Immunosuppression:
- 1st-line: high-dose steroids (response variable).
- Ciclosporin or tacrolimus for steroid-resistant cases (monitor nephrotoxicity).
- Other agents: cyclophosphamide, mycophenolate (selected cases).
- Supportive:
- ACE inhibitors / ARBs → reduce proteinuria and control BP.
- Lifestyle: weight reduction in obesity-related FSGS.
- Statins for dyslipidaemia.
- Anticoagulation if thrombosis risk high.
- Advanced disease: dialysis or renal transplantation (but beware recurrence).
📉 Prognosis
- Variable course: some remit, many progress to CKD/ESRD within 5–10 years.
- Poor prognostic factors: high baseline proteinuria, resistance to steroids, renal impairment at diagnosis.
📖 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery