Action Potential Neuron Versus Cardiac Ventricular Myocyte
⚡ Neuronal Action Potential (Fast Spike)
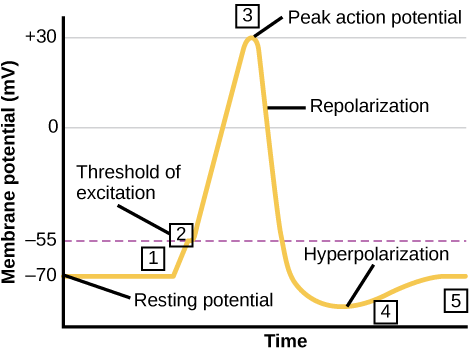
- Resting Membrane Potential (-70 mV): Maintained by the Na⁺/K⁺ ATPase (3 Na⁺ out, 2 K⁺ in) and K⁺ leak channels → inside of the cell remains negative relative to the outside.
- Threshold (~ -55 mV): If stimulus depolarises beyond threshold, voltage-gated Na⁺ channels open → an all-or-none response is triggered.
- Depolarisation (+30 mV peak): Massive Na⁺ influx through voltage-gated Na⁺ channels causes rapid upstroke. These channels then inactivate automatically.
- Repolarisation: Voltage-gated K⁺ channels open more slowly → K⁺ efflux restores negativity. Na⁺ channels remain inactivated until the cell repolarises.
- Hyperpolarisation: Excess K⁺ efflux makes the membrane more negative than resting (~ -80 mV), before leak channels and pumps re-establish baseline.
- Refractory Periods:
- Absolute refractory: No second AP possible (Na⁺ channels inactive).
- Relative refractory: A stronger stimulus needed during hyperpolarisation.
❤️ Cardiac Ventricular Action Potential (Phases 0–4)
Much longer (~200–400 ms) than neuronal APs, with a plateau that prevents tetany and synchronises contraction.
- Phase 4 (Resting): -90 mV, dominated by inward rectifier K⁺ current (IK1).
- Phase 0 (Rapid depolarisation): Fast Na⁺ influx through voltage-gated Na⁺ channels → steep upstroke (QRS complex on ECG).
- Phase 1 (Early repolarisation): Transient outward K⁺ current (Ito) produces a notch.
- Phase 2 (Plateau): Balance of inward Ca²⁺ current (ICaL via L-type channels) and outward K⁺ currents → sustained depolarisation allows Ca²⁺-induced Ca²⁺ release → excitation-contraction coupling.
- Phase 3 (Final repolarisation): Ca²⁺ channels close, K⁺ efflux (IKr, IKs) dominates → returns to -90 mV (T wave on ECG).
📊 Neuronal vs Cardiac Action Potentials
| Feature |
Neuron |
Cardiac Ventricular Myocyte |
| Duration |
~2 ms |
~200–400 ms |
| Threshold |
-55 mV |
-70 mV (ventricular); -40 mV (SA node) |
| Main Ion in Depolarisation |
Na⁺ influx |
Na⁺ influx (fast fibres); Ca²⁺ influx (nodal fibres) |
| Plateau Phase |
Absent |
Present (Ca²⁺ influx balances K⁺ efflux) |
| Refractory Period |
~1–2 ms (allows rapid firing) |
~200 ms (prevents tetany, ensures relaxation) |
| Clinical Relevance |
Local anaesthetics & toxins (lidocaine, tetrodotoxin) block Na⁺ → paralysis/anaesthesia. |
Antiarrhythmics target phases:
Class I (Na⁺), II (β-blockers), III (K⁺), IV (Ca²⁺).
|
🧩 Nodal vs Ventricular AP (Bonus)
- SA/AV node: Slow upstroke (phase 0 = Ca²⁺ influx), automaticity due to funny current (If, slow Na⁺ influx in phase 4). More dependent on Ca²⁺ channels than Na⁺.
- Ventricular cells: Sharp phase 0 (Na⁺), prominent plateau (phase 2), long refractory period.
💡 Clinical Pearls
- Neuronal AP:
- Lidocaine blocks fast Na⁺ channels → prevents nerve conduction.
- Tetrodotoxin (pufferfish) also blocks Na⁺ channels → fatal respiratory paralysis.
- Cardiac AP:
- Long refractory period protects against re-excitation → prevents tetanic contraction of the heart.
- Digitalis ↑ intracellular Ca²⁺ by blocking Na⁺/K⁺ ATPase → indirectly affects plateau & contractility.
- Arrhythmias often result from re-entry circuits exploiting heterogeneous refractory periods.
- ECG correlation:
- Phase 0 = QRS complex.
- Phase 2 = ST segment.
- Phase 3 = T wave.
🖼️ Diagrams
📖 Summary
Neuronal APs are fast, brief, and geared for rapid signalling. Cardiac APs are long, plateaued, and designed for coordinated contraction.
Understanding which ions dominate each phase underpins why different drugs (anaesthetics vs antiarrhythmics) work, and why pathology (e.g. multiple sclerosis, long QT syndromes) alters conduction and rhythm.
