
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Inguinal Hernia
⚠️ "Incarcerated" and "Strangulated" Inguinal Hernias are surgical emergencies.
ℹ️ About
- An inguinal hernia occurs when abdominal contents protrude through a weakness in the abdominal wall, usually via the inguinal canal.
- Contents may include peritoneum, fat, or small bowel.
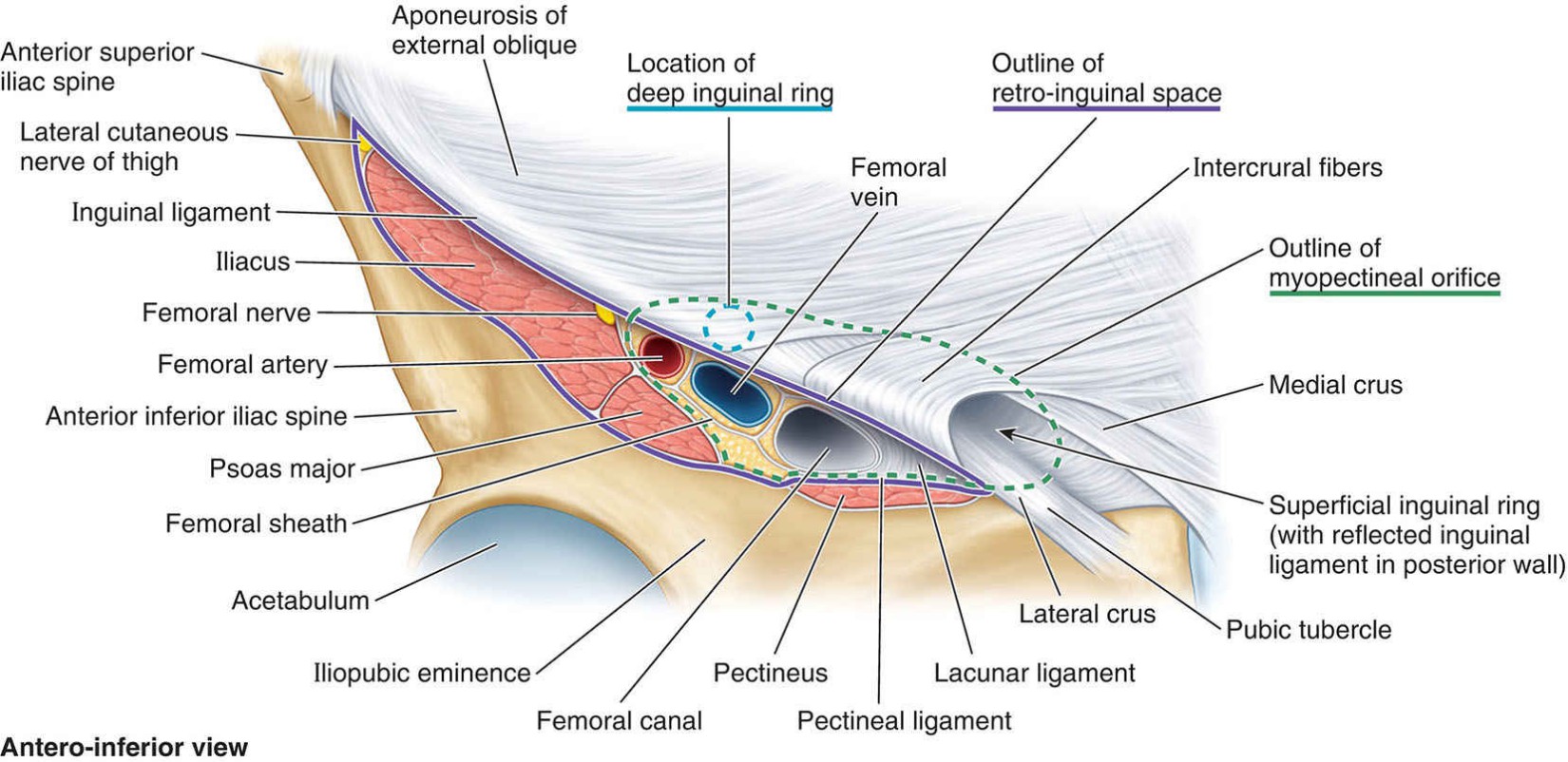
🔬Anatomy
Types of Inguinal Hernias
- Reducible: Contents can be pushed back into abdomen.
- Irreducible: Contents cannot be pushed back → risk of incarceration.
- Incarcerated: Trapped bowel, may obstruct.
- Strangulated: Blood supply compromised → ischaemia, necrosis.
Indirect vs Direct
- Indirect: Passes through deep inguinal ring, lateral to inferior epigastric vessels. Often congenital, may track into scrotum.
- Direct: Bulges through posterior wall of canal (Hesselbach’s triangle), medial to epigastric vessels. Usually acquired in older men.
Risk Factors
- Male sex (8× higher risk).
- Ageing, family history, previous pelvic surgery.
- Chronic raised intra-abdominal pressure (obesity, coughing, straining, heavy lifting).
- Connective tissue disorders.
🩺 Clinical Features
- Groin swelling above and medial to pubic tubercle, may extend to scrotum.
- Positive cough impulse.
- Pain/discomfort; tenderness or sudden severe pain suggests strangulation.
🔎 Investigations
- Bloods: FBC, U&E, CRP, group & save.
- Imaging: USS (useful in women/children), CT/MRI for diagnostic uncertainty, AXR if obstruction suspected.
💊 Management
- Emergency: ABCs, IV fluids, NBM, analgesia, antibiotics if strangulated → urgent surgical repair ± bowel resection.
- Elective: Most hernias benefit from repair (open or laparoscopic, mesh-based).
Surgical Approaches
- Open (Lichtenstein): Local or general anaesthetic; incision and mesh repair.
- Laparoscopic (TAPP/TEP): General anaesthetic, smaller scars, faster recovery.
⚠️ Complications
- Recurrence, wound infection, bleeding, chronic groin pain.
- General anaesthetic risks, DVT/PE.
- Rare: injury to cord structures, bladder, or bowel.
References
- Kenhub – Inguinal Hernia Anatomy
- NICE Guidance: Hernia – Surgical Management
📊 Comparison: Femoral vs Inguinal Hernias
| Feature | Femoral Hernia | Inguinal Hernia |
|---|---|---|
| 👥 Typical Patient | Older women (wider pelvis) | Young to middle-aged men |
| 📍 Location | Below inguinal ligament, lateral to pubic tubercle | Above inguinal ligament, medial or lateral to inferior epigastric vessels |
| 🧵 Neck of Hernia | Narrow → high risk of strangulation 🚨 | Wider → lower risk of strangulation |
| 🩺 Clinical Features | Small lump in groin, tender if incarcerated, often difficult to reduce | Groin lump enlarges on coughing/straining, often reducible |
| 🔎 Examination Clues | Swelling below & lateral to pubic tubercle | Swelling above & medial/lateral to pubic tubercle |
| ⚕️ Management | Urgent surgery due to strangulation risk | Elective repair unless obstructed/strangulated |
| 📉 Complications | Obstruction, strangulation, bowel necrosis | Less likely strangulation, but recurrence possible |
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery