Related Subjects:
|Polymerase chain reaction
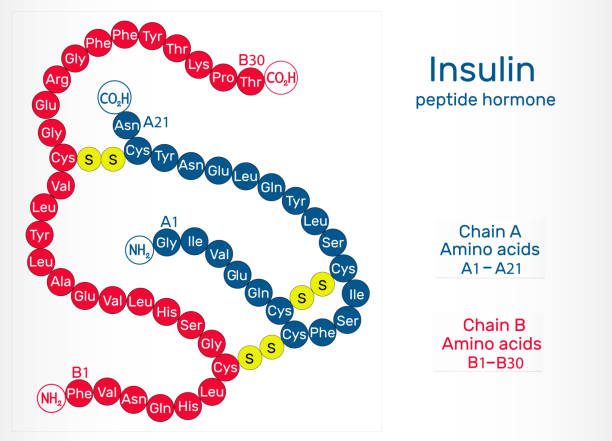
|Insulin Physiology
|Varicella Cerebral Vasculopathy
Insulin Physiology & Therapy – Updated Feb 2026
🧬 Insulin Production in Beta Cells
- Gene: INS on chromosome 11p15.5 → mRNA transcribed → exported to cytoplasm.
- Rough ER: Translation → pre-proinsulin (signal peptide cleaved → proinsulin).
- Golgi: Folding, disulfide bonds → packaged into immature secretory granules.
- Granules: Proinsulin cleaved by PC1/3 & PC2 → mature insulin + equimolar C-peptide (marker of endogenous production).
- Release: Into portal vein → ~50% first-pass hepatic extraction; remainder systemic circulation.
- Plasticity: Beta cells adapt dynamically (e.g., granule pools, transcription factors); recent 2025–2026 research highlights subpopulations for pulsatile/synchronised release.
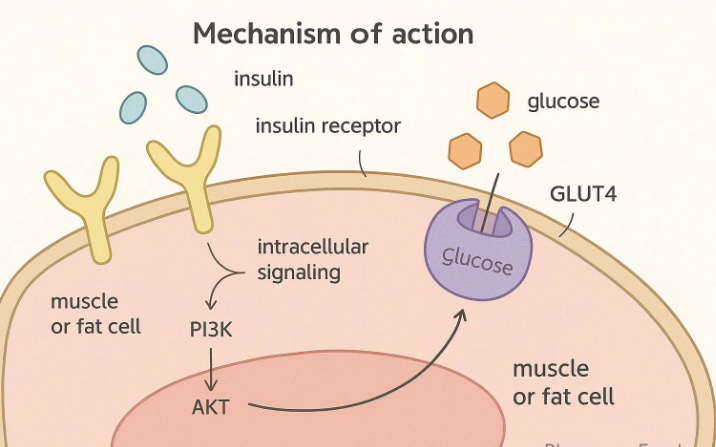
🧬 Insulin Receptor & Signaling
- Gene: INSR on chromosome 19p13.2 → heterotetramer (2α extracellular subunits bind insulin + 2β transmembrane subunits with tyrosine kinase domain).
- Binding: Conformational change → autophosphorylation of β subunits.
- Downstream: Phosphorylates IRS proteins → activates PI3K/AKT (metabolic: GLUT4 translocation, glycogenesis, lipogenesis, protein synthesis) and MAPK/ERK (mitogenic: proliferation).
- GLUT4 translocation: Key insulin action in muscle/adipose → ↑ glucose uptake.
🍬 Glucose Transporters (GLUTs) & Functions
- GLUT1: Basal/high-affinity; RBCs, brain, placenta, many cells (insulin-independent).
- GLUT2: Low-affinity, high-capacity, bidirectional; liver (glucose sensing/export), beta cells (glucose entry for insulin release), intestine/kidney.
- GLUT3: High-affinity; neurons, placenta (insulin-independent, supports high energy demand).
- GLUT4: Insulin-regulated; skeletal muscle, adipose tissue (translocates to membrane on insulin signaling → major peripheral glucose disposal).
🔄 Mechanism of Glucose-Stimulated Insulin Release (GSIS)
- Glucose enters beta cell via GLUT2 → glycolysis → ↑ ATP/ATP:ADP ratio.
- Closes ATP-sensitive K⁺ channels (K_ATP: Kir6.2 + SUR1) → membrane depolarisation.
- Opens voltage-gated Ca²⁺ channels → Ca²⁺ influx → exocytosis of insulin granules.
- Sulfonylureas close K_ATP independently → stimulate release.
- Amplifying pathways (e.g., GLP-1/cAMP, glutamate) enhance exocytosis.
📈 Insulin Release Patterns
- Biphasic GSIS: First phase (rapid, ~10 min): Release of docked/ready granules (Ca²⁺-dependent).
- Second phase (sustained): Mobilisation/reserve granules; amplified by metabolic signals.
- Basal: Pulsatile/low-level release; prandial peaks mimic natural pattern.
- Therapy goal: Basal-bolus/pumps replicate biphasic + basal secretion.
💉 Indications for Insulin Therapy
- Type 1 DM: Absolute requirement (prevent DKA); start immediately at diagnosis.
- Type 2 DM: When lifestyle/oral agents fail (HbA1c targets individualised); acute illness, peri-op, pregnancy, steroids, severe hyperglycaemia.
🩺 Insulin Administration Methods & Regimens (NICE NG28 2026-aligned)
- Basal-bolus (MDI): Long-acting basal (1–2× daily) + rapid-acting bolus pre-meals; preferred Type 1; flexible carb counting.
- Twice-daily biphasic/pre-mixed: Convenient for stable T2DM/Type 1 with regular lifestyle.
- Once-daily basal: Common T2DM initiation (add to metformin); simplify in frailty.
- Continuous subcutaneous insulin infusion (CSII/pump): Selected Type 1 (poor control, nocturnal hypos); with CGM.
- Syringe driver/IV infusion: Hospital/ICU/peri-op tight control.
💊 Types of Insulin (UK 2026: analogues preferred where benefit; biosimilars cost-effective)
- Rapid-acting (bolus): Lispro (Humalog), Aspart (Novorapid/Fiasp), Glulisine; onset 10–15 min, peak 1–2 h, duration 3–5 h.
- Short-acting (soluble): Actrapid/Humulin S; less used now.
- Intermediate (NPH/isophane): Insulatard/Humulin I; peak 4–12 h; cost-effective basal.
- Long-acting analogues: Glargine (Lantus/Semglee biosimilar), Detemir (Levemir – phasing out late 2026), Degludec (Tresiba – ultra-long, flexible timing).
- Premixed/biphasic: NovoMix 30/Humalog Mix25/50; 30–50% rapid + 50–70% intermediate.
Cases - Insulin Management Examples
- Case 1 – New T1DM 💉: 16M weight loss/polyuria/ketosis, HbA1c 96. Rx: Basal-bolus (glargine + aspart), carb counting, DAFNE education.
- Case 2 – T1DM adjustment 🍽️: 25F frequent postprandial highs. Rx: Optimise carb:insulin ratio, CGM review.
- Case 3 – T2DM initiation ⚠️: 60M max OADs, HbA1c 85, fasting >12. Rx: Once-daily basal (NPH/glargine) + metformin continuation.
- Case 4 – Frailty simplification 👴: 82F recurrent hypos/falls, HbA1c 49. Rx: Simplify to once-daily basal, avoid over-treatment.
- Case 5 – Pump therapy ⚙️: 34M nocturnal hypos/poor control on MDI. Rx: CSII + CGM.
Teaching Point 🩺:
Type 1: Insulin-dependent from diagnosis; basal-bolus/pump + carb counting standard.
Type 2: Insulin when OADs fail/acute need; individualise (continue metformin, simplify in frailty, prefer analogues/biosimilars).
Mimic physiology: Basal for fasting; bolus for meals; monitor hypos/risks.
NICE NG28 (2026): Shared decisions, sick-day rules, CV/renal benefits first.
📚 References (Feb 2026)
- NICE NG28 Type 2 Diabetes (updated Feb 2026): Insulin sections refreshed.
- BNF Insulin Summary (2026): Analogue preference, biosimilars.
- Recent reviews: Biphasic GSIS (eLife 2024; Cell Metab 2025); GLUT functions (2025).
