Related Subjects:
| Achalasia
| Oesophageal Carcinoma
| Diffuse Oesophageal Spasm
| Oesophageal Perforation (Rupture)
| Gastro-Oesophageal Reflux Disease
| Barrett’s Oesophagus
| Upper Gastrointestinal Bleed
| Oesophageal Variceal Bleeding
| Dieulafoy Lesion
| Peptic Ulcer Disease
| Oesophagogastroduodenoscopy (OGD/EGD)
| Hereditary Haemorrhagic Telangiectasia
🩸 Oesophageal Variceal Bleeding - Comprehensive Management (Makindo)
⚠️ Medical Emergency: Acute variceal haemorrhage carries a 30–50% mortality per bleed.
Management is time-critical: treat on suspicion, not confirmation. Terlipressin + antibiotics + restrictive transfusion should be started immediately. Endoscopy stops the bleed - vasoconstriction buys survival.
📖 Background
- Oesophageal varices result from portal hypertension, most commonly due to cirrhosis.
- Portal hypertension causes dilation of submucosal oesophageal veins, which rupture under high pressure.
- Bleeding is often brisk, recurrent, and haemodynamically catastrophic.
🧬 Pathophysiology (Why these treatments work)
- Normal portal pressure: < 6 mmHg
- Varices form: ≥ 10 mmHg
- Bleeding risk rises sharply: ≥ 12 mmHg
- Splanchnic vasodilatation (NO-mediated) ↑ portal inflow.
- Vasoactive drugs ↓ portal venous inflow → ↓ variceal wall tension.
🚑 Initial Resuscitation (ABCD first)
- Airway: Early intubation if massive haematemesis, encephalopathy, or shock.
- Breathing: High-flow oxygen.
- Circulation:
- 2 × large-bore IV cannulae.
- Cautious crystalloid boluses.
- Restrictive transfusion: target Hb 7–8 g/dL.
- Avoid over-transfusion (↑ portal pressure → rebleeding).
- Disability: Assess encephalopathy.
🧪 Investigations
- FBC, U&E, LFTs, clotting, lactate.
- Group & crossmatch (≥ 6 units if unstable).
- ABG if shocked or encephalopathic.
- Urgent OGD once stabilised (within 12 hours).

💊 Pharmacological Therapy (Start Immediately)
🔹 Vasoactive Therapy
- Terlipressin (first-line in UK)
- 2 mg IV every 4 hours for first 48 hours
- Then 1 mg IV every 4 hours
- Total duration: 3–5 days (stop after haemostasis achieved)
- Mechanism: Splanchnic vasoconstriction → ↓ portal inflow.
- Contraindications / caution: IHD, severe PVD, uncontrolled hypertension, arrhythmias.
🔹 Antibiotic Prophylaxis (MANDATORY)
- Why: Bacterial translocation increases rebleeding and mortality.
- IV Ceftriaxone (preferred in UK):
- 1 g IV once daily for 7 days
- Especially Child–Pugh B or C
- Alternatives:
- Norfloxacin 400 mg PO BD × 7 days
- Ciprofloxacin 500 mg PO BD × 7 days
🔹 Encephalopathy Prevention
- Lactulose: 20–30 mL PO/NG TDS
- Titrate to 2–3 soft stools/day
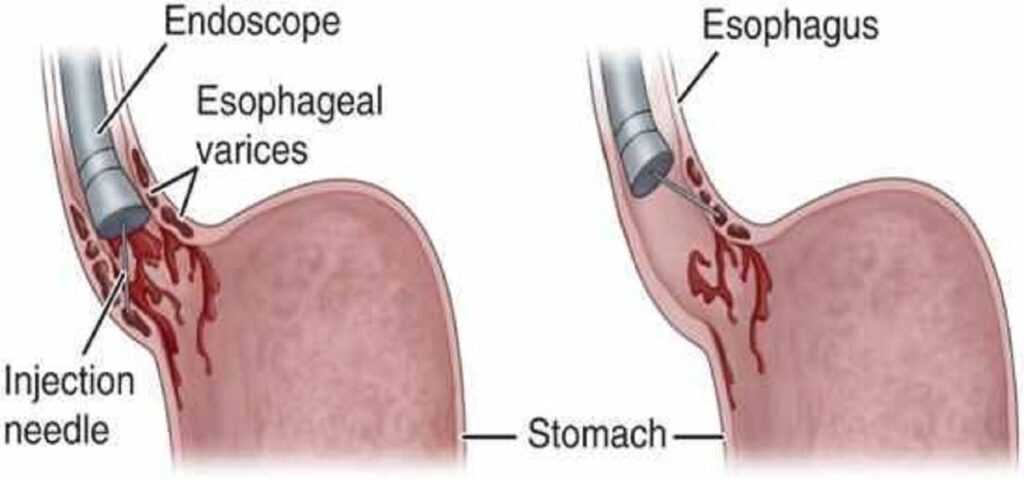
🎯 Endoscopic Therapy (Definitive)
- Endoscopic variceal band ligation - treatment of choice.
- Sclerotherapy if banding not feasible.
- Achieves haemostasis in ~90% when combined with drugs.
🚨 Salvage / Rescue Therapy
- Balloon tamponade (Sengstaken–Blakemore or Minnesota tube)
- Temporary bridge only
- Maximum 24 hours
- High risk: aspiration, oesophageal necrosis
- TIPS (Transjugular Intrahepatic Portosystemic Shunt)
- Indicated for refractory or recurrent bleeding
- Creates low-resistance channel between portal and hepatic veins
- Risk: hepatic encephalopathy
🛡️ Secondary Prophylaxis (After Acute Bleed)
- Non-selective β-blockers
- Propranolol 20–40 mg BD (titrate to HR 55–60)
- Carvedilol 6.25 mg OD → 12.5 mg OD
- Repeat endoscopic band ligation every 2–4 weeks until eradication.
- Optimise cirrhosis management (alcohol abstinence, nutrition, surveillance).
💡 Exam & On-Call Pearls
- Cirrhotic + haematemesis = variceal bleed until proven otherwise.
- Do not wait for endoscopy to start terlipressin and antibiotics.
- Normal Hb early does not exclude massive bleeding.
- Terlipressin is the only vasoactive drug shown to improve survival.
