Influenza
Influenza is an acute viral respiratory infection caused by Orthomyxoviridae viruses.
It remains a major cause of global morbidity and mortality, with significant health, social, and economic impacts.
Epidemics occur seasonally, while pandemics arise from new influenza A subtypes.
- Types of Influenza:
- 🅰️ Influenza A: Multiple animal reservoirs (birds, pigs). Causes pandemics via antigenic shift (e.g. 1918, 2009 H1N1).
- 🅱️ Influenza B: Only humans; less severe, seasonal outbreaks. Still significant in children.
- 🇨 Influenza C: Mild, self-limiting, rarely causes outbreaks.
- 🇩 Influenza D: Emerging, mainly cattle; not yet a proven human pathogen.
🧬 Virology: Antigenic Drift and Shift
- Antigenic Drift: Gradual point mutations in Haemagglutinin (H) and Neuraminidase (N). Explains why seasonal flu vaccines need yearly updates.
- Antigenic Shift: Abrupt reassortment between strains (e.g. bird + pig + human). Creates novel subtypes with little human immunity → pandemics.
📡 Transmission and Spread
- Spread via droplets, aerosols, and fomites.
- Contagious from 1–2 days before symptoms until ~7 days after (longer in children or immunocompromised).
- Closed settings (care homes, schools, prisons) accelerate outbreaks.
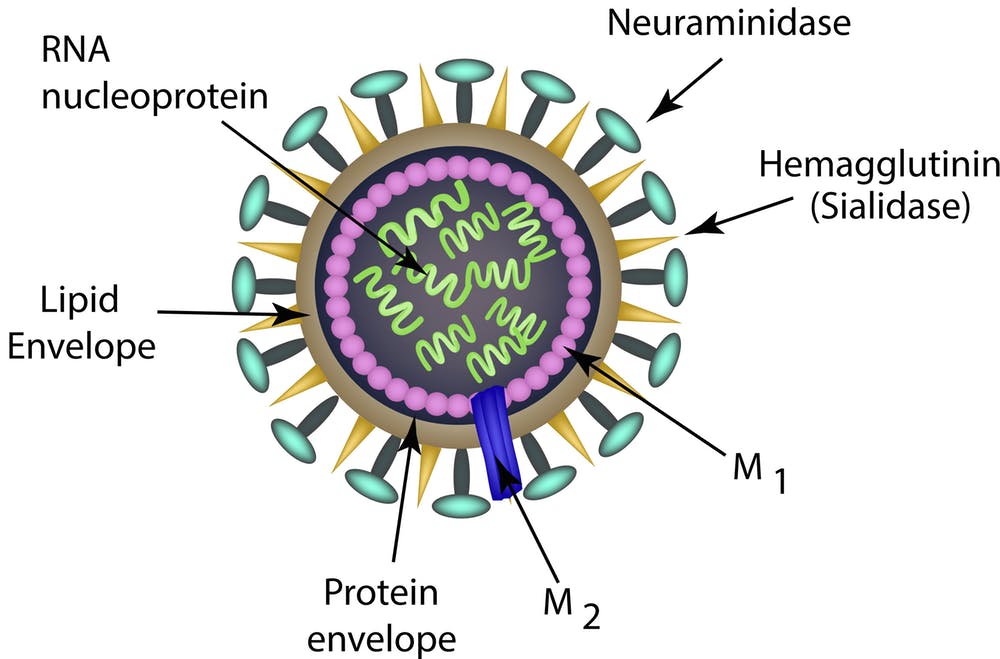
🔬 Viral Structure
- Haemagglutinin (H) → binds host epithelial cells (entry).
- Neuraminidase (N) → cleaves sialic acid to release new virions (spread).
- Other proteins (M2, NS1) target host immunity - basis for some antiviral drugs.
🤒 Clinical Presentation
- Rapid onset: high fever, chills, myalgia, headache, cough, sore throat, fatigue.
- Children: often vomiting, abdominal pain, febrile seizures.
- Adults: high absenteeism, prolonged fatigue (“post-viral syndrome”).
⚠️ Complications
- Pneumonia: Viral or secondary bacterial (esp. S. pneumoniae, S. aureus).
- Cardiac: Myocarditis, arrhythmias, heart failure exacerbation.
- Neurological: Guillain-Barré, encephalitis, acute necrotising encephalopathy (rare, severe in children).
- Exacerbations: COPD/asthma flare-ups, decompensated diabetes.
🧪 Investigations
- RT-PCR: 🥇 Gold standard for diagnosis (nasopharyngeal swab).
- Rapid antigen tests: Point-of-care, less sensitive.
- Chest X-ray: Indicated if pneumonia suspected.
💊 Management
- Supportive care: Rest, hydration, paracetamol/NSAIDs, oxygen if hypoxic.
- Antivirals (best if started ≤48h from onset):
- 💊 Oseltamivir (Tamiflu): Oral, 75 mg BD x 5d.
- 💨 Zanamivir: Inhaled, useful in Oseltamivir resistance.
- 💉 Peramivir: IV option (severe cases, limited use in UK).
- 🧬 Baloxavir: Newer single-dose cap-dependent endonuclease inhibitor (licensed in Japan/US, not yet routine in UK).
- Prophylaxis: Antivirals for vulnerable contacts during outbreaks (care homes, oncology wards).
- Hospitalisation: For hypoxia, severe pneumonia, or vulnerable high-risk patients.
💉 Prevention and Vaccination
- Annual influenza vaccination: Updated seasonally based on WHO global surveillance.
- Priority groups: Elderly, pregnant women, children (UK nasal spray programme), healthcare workers, immunocompromised, chronic illness patients.
- 🧼 Hygiene: handwashing, masks in outbreaks, respiratory etiquette.
- COVID-19 lessons: Flu + COVID co-infection worsens outcomes → dual vaccination campaigns now common in UK.
📊 Public Health & Modern Considerations
- 🛰️ WHO Global Influenza Surveillance and Response System (GISRS) monitors strains for vaccine design.
- 📉 Economic burden: lost productivity + NHS winter pressures.
- 🌍 Emerging zoonotic threats: Avian flu (H5N1, H7N9) & swine flu (H1N1) highlight pandemic risk.
- 📦 Stockpiles of antivirals and PPE remain part of UK’s national preparedness strategy.
🧑⚕️ Teaching Point
Think of influenza not just as a seasonal illness, but as a global health threat with pandemic potential.
Always consider secondary bacterial pneumonia if a patient initially improves then deteriorates.
Vaccination + early antiviral use in high-risk groups saves lives.
