
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Burns Management Guide
Related Subjects: |Cellulitis |Pyoderma gangrenosum |Pemphigus Vulgaris |Toxic Epidermal Necrolysis |Stevens-Johnson Syndrome |Necrotising fasciitis |Gas Gangrene (Clostridium perfringens) |Purpura Fulminans |Severe burns |Anatomy of Skin
| 🛠️ Initial Management of Severe Burns: Always Look for Secondary Injuries |
|---|
|
🔥 Anyone with burns should also be presumed to have smoke inhalation injury - consider the ABCs and watch for stridor, hoarseness, or drooling. 😮💨 These patients are at risk for ARDS and airway compromise, which may require early intubation. 📞 Referral: Transfer to a burns centre if:
- 👶 >10% TBSA in children
- 🧑 >15% TBSA in adults
- 🩹 Any full-thickness burns
- 😷 Burns to face, hands, perineum, feet, flexures, or joints
- ⚡ Chemical, electrical, lightning injuries
- 🔥 Circumferential limb or chest burns
- 🚨 Suspected inhalation injury
🔥 Types of Burns
- ☀️ First Degree / Superficial: Epidermis only. Red, painful, no blisters. Heal without scarring.
- 💧 Second Degree / Partial Thickness: Epidermis + dermis. Red, blistered, very painful, moist. Heal with minimal scarring.
- 🪵 Third Degree / Full Thickness: All layers destroyed. White/charred/leathery. Painless (nerve damage). Needs grafting → scarring.
😷 Signs of Inhalational Injury
- Facial/neck/chest burns
- Singed nasal hair/eyebrows
- Soot in sputum/oropharynx
- Hoarseness, stridor, dyspnoea
- Oropharyngeal swelling/erythema
⚠️ Complications of Burns
- Compartment syndrome
- Hypovolaemia, electrolyte imbalance
- Infection, sepsis
- Hypothermia
- Neuropathic pain, pruritus
- Hypertrophic scars, contractures
- Psychological trauma: depression, anxiety, PTSD
📍 Special Areas of Concern
- Face, hands, perineum, genitalia, feet, flexures, joints → functional & cosmetic impact.
🧪 Investigations
- Bloods: FBC, U&E, glucose, clotting, CK, cross-match
- ABG: lactate, HbCO
- CXR if inhalation suspected
🧾 Management Overview
- ABCDE approach 🔄
- High-flow O₂ 💨
- Fluid resuscitation 💧 (Parkland + urine monitoring)
- Early intubation if airway risk 🫁
- Wound care: cling film, sterile dressings 🩹
- IV analgesia 💊
- Nutritional support 🍲 (↑ metabolic demand, dietician input)
- Escharotomy if needed ✂️
- Tetanus prophylaxis 💉
- Early burns unit referral 📞
📚 Teaching Commentary
Burns are a multisystem insult - airway, circulation, and metabolism all collapse if not managed promptly. The first 24h = airway + fluids, not definitive surgery. Always check for “hidden killers”: inhalational injury, CO or cyanide, associated trauma. UK practice: 🔗 burns care is regionalised → early referral is life-saving. Remember: 🧪 resuscitation is a balance - underdo it and they die of shock, overdo it and you worsen oedema, including airway swelling. And never forget the patient’s psychological and safeguarding needs - scarring and trauma can last far beyond the acute injury.
🔖 References
- ABC of Burns: Pathophysiology and Types of Burns
- Clinical Guideline: Burns Injury
- Management of Major Burns: A Review
Case 1 – Adult flame burn with inhalation risk
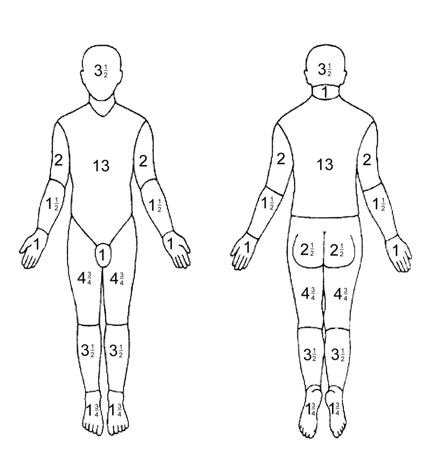
A 38-year-old rescued from a house fire has facial burns, singed nasal hairs, hoarse voice, and cough with soot; mixed-depth burns to the anterior trunk and both upper limbs (~28% TBSA, Rule of Nines). Priorities: ABCDE with high-flow O₂ (100% non-rebreathe), early airway protection if progressive oedema/stridor, and blood gases including carboxyhaemoglobin (pulse oximetry unreliable). Start warmed IV fluids using the Parkland formula (4 mL/kg/%TBSA of lactated Ringer’s; give half in 8 h from time of burn), titrating to urine ≥0.5 mL/kg/h; insert urinary catheter and consider analgesia, tetanus, and escharotomy if circumferential chest/limb burns impair ventilation/flow. Cool the burn (20 min tepid water if <3 h from injury), cover with cling film, avoid ice. Refer to a UK burns centre (e.g., >10% TBSA, face/airway, hands/perineum, electrical/chemical, or inhalation injury) for debridement and definitive dressings/grafting.
Case 2 – Paediatric scald; safeguarding considerations
A 2-year-old pulls a kettle lead causing hot-water scald to the anterior chest and left arm; blistered, painful partial-thickness burns covering ~8% TBSA (use Lund–Browder chart). Manage with ABCDE, prompt analgesia (oral morphine/IN fentanyl as appropriate), tepid cooling for up to 20 min, non-adherent dressing (paraffin gauze) and cling film, elevation of the limb, and oral fluids ± IV if not tolerating; consider fluid resuscitation if >10% TBSA (many UK centres use 2–3 mL/kg/%TBSA in children) and maintain euglycaemia. Assess tetanus status. Document a careful history and injury pattern; involve senior review and safeguarding if concerns (e.g., clear immersion lines, inconsistent story). Arrange burns clinic follow-up within 24–48 h to monitor pain, infection, and function; early physiotherapy/splinting if joints are involved.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery