Related Subjects:
|Fractured Neck of Femur
|Fractured Shaft Femur
|Supracondylar Femur Fractures
|Supracondylar Humerus Fractures
|Femoral fractures
|Fractured Tibia and Fibula
|Pelvic fractures
Humerus Fractures 💪🦴 are common injuries, particularly in older adults with osteoporosis.
Key priorities: neurovascular assessment (radial & axillary nerves, brachial artery) and appropriate referral.
If there are neurological/vascular deficits or joint involvement → urgent orthopaedic input.
📖 About
- Neck of Humerus Fractures: common in elderly, usually after a fall on an outstretched hand (FOOSH); associated with degenerative bone disease.
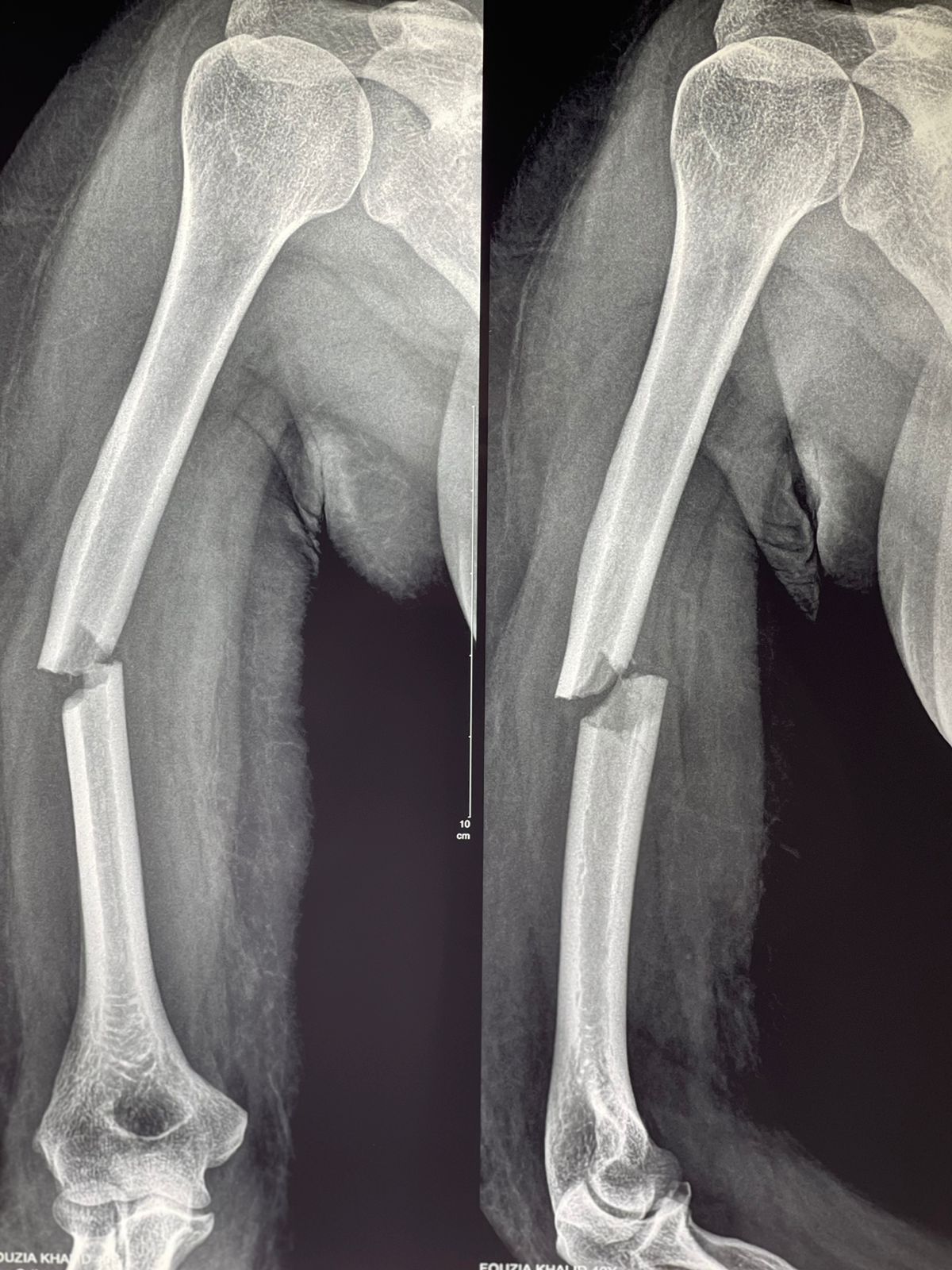
- Shaft of Humerus Fractures: often rotational injuries (e.g. arm wrestling); also seen in metastatic disease. ⚠️ Assess and document radial nerve function (wrist extension + sensation in 1st web space).
⚙️ Aetiology
- Trauma (falls, direct blow, arm-wrestling)
- Osteoporosis
- Paget’s disease
- Pathological fractures (e.g. metastases)
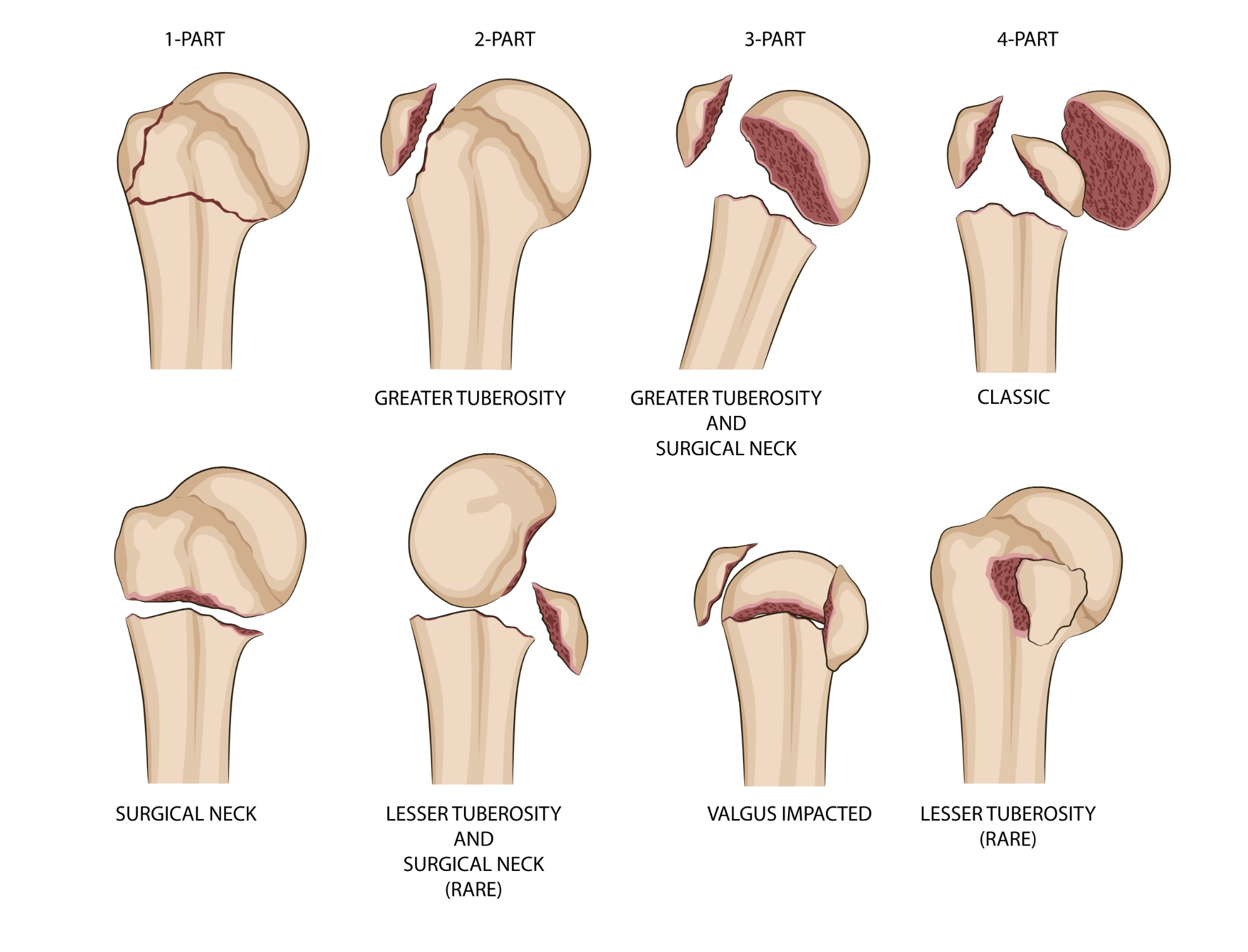
- May involve: greater tuberosity, lesser tuberosity, anatomical neck, surgical neck
🩺 Clinical Features
- Localised pain, swelling, tenderness; arm may hang limply with bruising.
- ⚡ Neurovascular exam:
- Radial nerve: wrist extension + sensation in 1st dorsal web space.
- Axillary nerve: sensation over regimental badge area + deltoid power.
- Brachial plexus screen + distal neuro exam.
- Check radial pulse & perfusion.
🔎 Types
- Proximal humerus: FOOSH, seizures, direct trauma; older patients; axillary nerve vulnerable.
- Midshaft: commonly affects radial nerve (spiral groove injury).
🧪 Investigations
- Bloods: FBC, ESR, U&E, Ca (esp. if pathological fracture suspected).
- Imaging:
- X-ray: humerus AP, scapular Y, axillary views.
- CT if complex or intra-articular involvement.
⚠️ Complications
- Nerve injuries:
- Axillary nerve → proximal fractures.
- Radial nerve → midshaft fractures.
- Suprascapular & musculocutaneous less common.
- Vascular injury: axillary or brachial artery (expanding mass, absent pulses).
- Avascular necrosis: humeral head after complex or anatomical neck fractures.
- Malunion, stiffness, rotator cuff injury.
- Fracture dislocations.
💊 Management
- General: Analgesia, sling/immobilisation, neurovascular monitoring, fracture clinic referral.
- Proximal (neck of humerus):
- Most are undisplaced → conservative (collar & cuff or sling; allow gravity traction).
- Physiotherapy + analgesia.
- Shaft of humerus:
- 2-part fracture: humeral brace, post-reduction X-ray, fracture clinic.
- 3+ part fracture / unstable: brace + urgent orthopaedic referral (possible fixation).
- Always re-document radial nerve status.


🚨 Surgical Emergencies
- Open fractures.
- Associated with shoulder dislocation.
- Combined injuries (e.g. ipsilateral forearm fracture → “floating elbow”).
- Anatomical neck fractures (high AVN risk).
- Neurovascular compromise not resolving with reduction.
📌 OSCE / Exam Pearls
- Always document radial & axillary nerve function before and after any intervention.
- Look for expanding swelling = axillary artery injury.
- Most proximal humeral fractures in elderly = sling + analgesia; surgical if displaced/complex.
- Radial nerve palsy in closed shaft fractures often recovers spontaneously → observe unless open fracture.
📚 References
- Rockwood & Green’s Fractures in Adults, 9th ed.
- NICE: Non-complex fractures (NG38). 2016.
- British Orthopaedic Association: BOAST guidelines on humeral fractures.
