
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Granulomatosis with Polyangiitis GPA (Wegeners)✅
Related Subjects: Granulomatosis with Polyangiitis (GPA, formerly Wegener's) | Goodpasture's Syndrome (Anti-GBM Disease) | Respiratory Failure | Acute Kidney Injury
Early recognition and prompt immunosuppression are critical to prevent irreversible organ damage. If GPA is suspected, urgently request c-ANCA (PR3). Without treatment, GPA can destroy kidneys within weeks.
ℹ️ Overview
- 🧑⚕️ First described by Dr. Friedrich Wegener in 1936 (now renamed GPA due to historical associations).
- 📛 Granulomatosis with Polyangiitis (GPA) is a systemic necrotizing vasculitis affecting ENT, lungs, and kidneys.
- ⏱️ Untreated mortality: ~90% within 2 years.
🧬 Pathophysiology
- 🌡️ Autoimmune, small-to-medium vessel vasculitis, likely triggered by environmental antigens.
- 🦠 Staphylococcus aureus carriage increases relapse risk; eradication reduces recurrence.
- 🩺 Renal involvement: 40% at presentation, up to 90% over disease course.
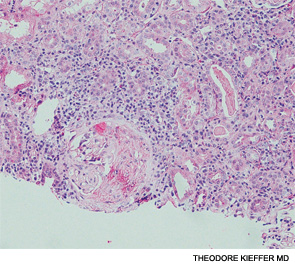
- 🪢 Granulomatous inflammation → necrosis of affected tissues (ENT, lungs, kidneys).
📊 Epidemiology
- 👥 Incidence ~3/100,000 (USA); similar UK estimates.
- ⏱️ Mean age of onset ~50 yrs.
- ⚖️ M:F ratio = 1:1.
- 🌍 Predominantly Caucasian populations (~90%).
🧱 Granuloma Formation
🩺 Clinical Features
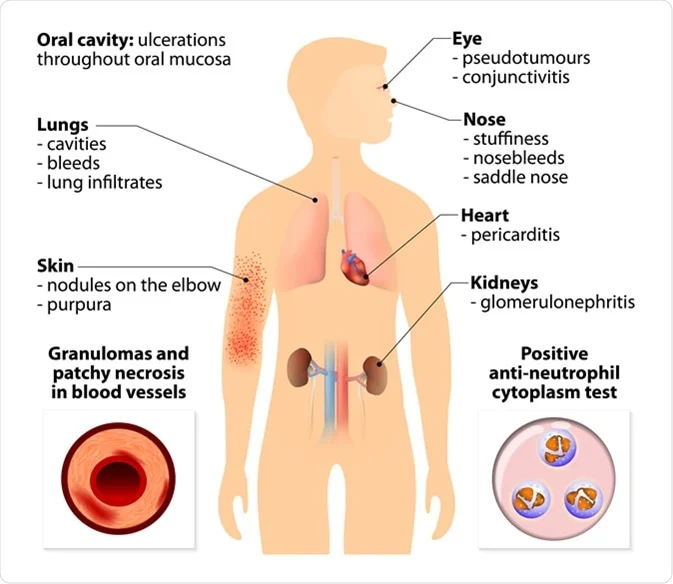
- 🛏️ Constitutional: fever, night sweats, malaise, fatigue.
- 👃 ENT: chronic sinusitis, epistaxis, otitis media, nasal septal perforation, saddle nose deformity.
- 🫁 Lungs: cough, haemoptysis, pulmonary haemorrhage (↑DLCO), nodules ± cavitation.
- 🧽 Kidneys: hypertension, haematuria, pauci-immune necrotizing glomerulonephritis.
- 👁️ Ocular: uveitis, scleritis, proptosis.
🔬 Investigations
- 🩸 FBC: anaemia, leukocytosis.
- 🧪 U&E: rising creatinine/urea; renal impairment.
- 🔥 ESR/CRP: elevated.
- 🧪 Complement: sometimes low.
- 🫁 CXR: nodules, infiltrates, cavitations, pulmonary haemorrhage.
- 🧫 Urinalysis: proteinuria, haematuria, dysmorphic RBCs, RBC casts.
- 🖥️ HRCT chest: alveolar haemorrhage, nodules, airway stenosis.
- 🔑 ANCA serology: c-ANCA (PR3) positive 80–90% (correlates with activity), p-ANCA (MPO) positive 10–20%.
- 🔍 Biopsy (ENT/lung/kidney): necrotizing granulomatous vasculitis.
- 🫁 BAL: blood in alveoli for pulmonary haemorrhage.
- 💨 DLCO: increased in alveolar haemorrhage due to Hb CO-binding.
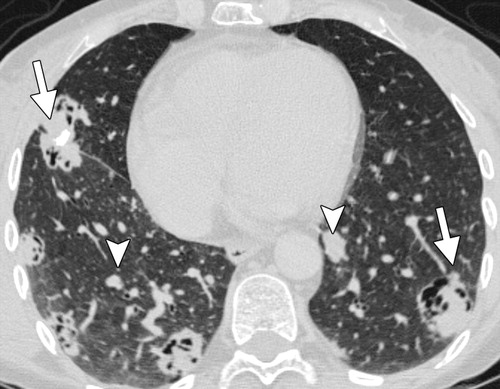
🖼️ Imaging
📸 CT: multiple cavitary (arrows) and non-cavitary (arrowheads) pulmonary nodules typical of GPA.
💊 Management
- ⚠️ Untreated mortality ~90% at 2 years; early treatment dramatically improves survival.
- Induction therapy: • Severe/organ-threatening: high-dose corticosteroids + cyclophosphamide (CYC) or rituximab (RTX). • Non-severe: methotrexate (MTX) or RTX ± steroids.
- Maintenance therapy: azathioprine, MTX, or RTX (especially PR3+ high-risk relapsers). • RTX infusions can extend up to 42 months for high relapse risk.
- Adjunctive therapy: • Co-trimoxazole prophylaxis (for Pneumocystis and reduces Staph. nasal colonisation). • Long-term mupirocin nasal therapy. • Plasma exchange (PLEX) if severe renal disease (Cr >500 μmol/L) or pulmonary haemorrhage.
Case – Granulomatosis with Polyangiitis (GPA)
42M with chronic sinusitis, epistaxis, conductive hearing loss, pleuritic chest pain, blood-streaked sputum, fatigue, and ankle oedema. Exam: saddle nose, crackles; BP 158/92. Labs: normocytic anaemia, rising creatinine, RBC casts; CXR: multiple cavitating nodules. Serology: strongly positive c-ANCA (PR3). Nasal/renal biopsy: necrotising granulomatous vasculitis. Management: IV methylprednisolone → high-dose oral taper + rituximab (or cyclophosphamide), PPI, bone protection, PJP prophylaxis. Consider plasmapheresis if severe pulmonary haemorrhage or dialysis-dependent RPGN. Maintenance with rituximab/azathioprine; multidisciplinary follow-up (ENT, respiratory, nephrology). Monitor for relapse and treatment toxicity. Differentials: microscopic polyangiitis, EGPA, infection (TB/fungal), malignancy.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery