Tilt Table Testing in Reflex Syncope
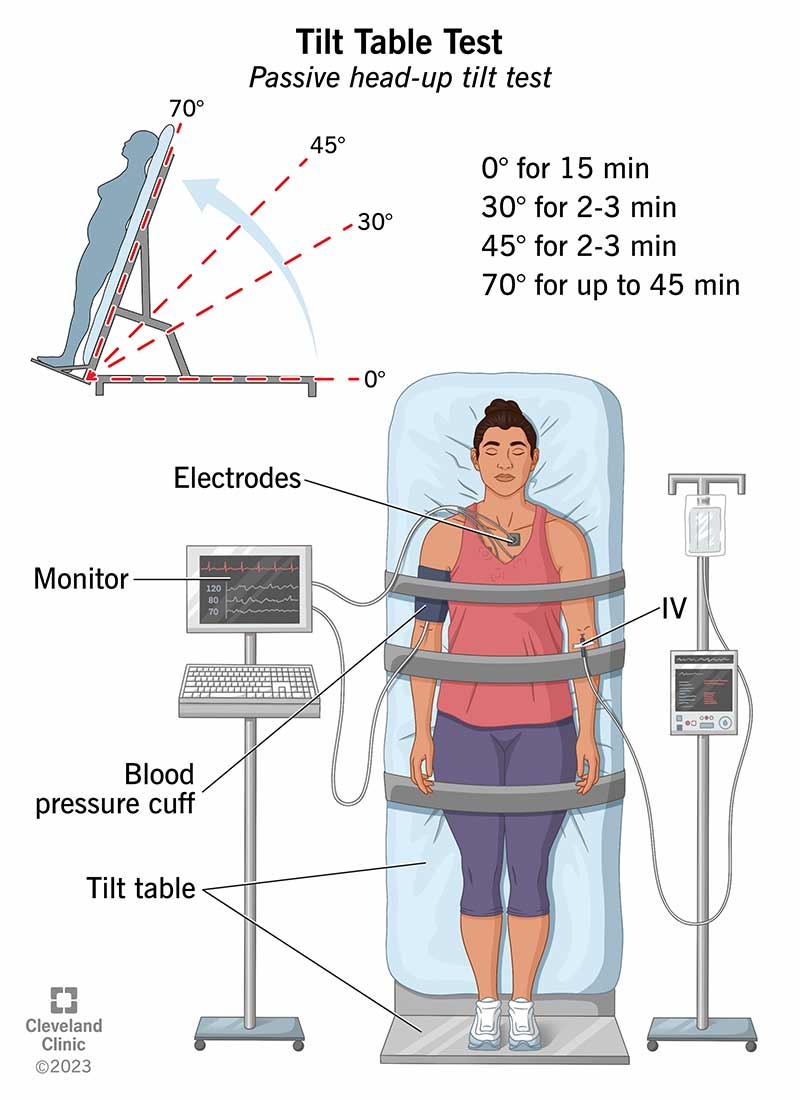
Tilt table testing is used to reproduce syncope under controlled conditions while monitoring heart rate and blood pressure. It helps identify whether reflex syncope is mainly due to bradycardia, vasodilation, or a mixed response. NICE advises that tilt testing should not be used routinely when vasovagal syncope is already clear from the history, but it may be considered in recurrent troublesome syncope where identifying a severe cardioinhibitory response would change management.
⚙️ Pathophysiology
Reflex syncope occurs when autonomic reflexes cause inappropriate vasodilation and/or vagal activation. Vasodilation reduces venous return and cardiac output, while vagal activation can slow the sinus node or cause transient asystole. The clinical result is cerebral hypoperfusion, causing presyncope or transient loss of consciousness.
📋 When to consider tilt table testing
- Recurrent syncope causing injury, anxiety, occupational risk or reduced quality of life.
- Suspected reflex syncope where the diagnosis remains uncertain after initial assessment.
- Assessment of whether syncope has a marked cardioinhibitory component.
- Selected patients where results may guide treatment, education or pacing decisions.
🚫 When tilt testing is less useful
- Clear simple vasovagal syncope diagnosed from the history.
- Syncope with high-risk cardiac features requiring urgent cardiac assessment instead.
- Unexplained syncope before appropriate ECG monitoring has been considered.
📊 Tilt table responses in reflex syncope
| Type |
Response |
Definition |
Treatment |
| Type 1 |
Mixed cardioinhibitory and vasodepressor |
Heart rate falls, but not to < 40 bpm. |
Cardiac pacing may be considered in selected cases, but is less effective when there is an important vasodepressor component.
|
| Type 2A |
Cardioinhibitory without asystole |
Heart rate < 40 bpm for > 10 seconds. |
Cardiac pacing may be considered, particularly in carotid sinus hypersensitivity rather than typical vasovagal syncope.
|
| Type 2B |
Cardioinhibitory with asystole |
Asystole > 3 seconds with symptoms. |
Cardiac pacing may be considered in selected patients, especially older patients with recurrent, unpredictable, injurious episodes and documented cardioinhibitory syncope.
|
| Type 3 |
Vasodepressor |
Fall in systolic blood pressure > 50 mmHg with symptoms. Heart rate does not fall by more than 10% from its peak at the time of syncope.
|
Often harder to treat. Options include education, trigger avoidance, hydration, salt intake if appropriate, compression hosiery and, in selected cases, fludrocortisone.
|
💊 Treatment principles
- Education: explain the benign mechanism, warning symptoms and how to lie down early.
- Trigger avoidance: avoid dehydration, prolonged standing, overheating and missed meals.
- Physical counter-pressure manoeuvres: leg crossing, squatting, hand gripping or tensing muscles during prodrome.
- Volume support: encourage fluids and salt where clinically appropriate, avoiding this in heart failure, severe hypertension or advanced kidney disease.
- Compression hosiery: may help patients with a vasodepressor or orthostatic component.
- Medication: fludrocortisone may be considered in selected patients, but evidence is limited and monitoring for hypertension, oedema and hypokalaemia is needed.
- Cardiac pacing: reserved for carefully selected patients with a dominant cardioinhibitory mechanism, especially carotid sinus hypersensitivity or documented asystolic syncope.
🩺 Clinical interpretation
The key question is whether the patient faints because the heart slows, the blood pressure falls, or both. Pacing can treat bradycardia or asystole, but it cannot correct profound vasodilation; this is why pacing is less effective in mixed or vasodepressor syncope. In vasodepressor syncope, treatment focuses on improving venous return, blood volume and early recognition of prodromal symptoms.
⚠️ Red flags suggesting cardiac syncope
- Syncope during exertion.
- Syncope while lying flat.
- Palpitations immediately before syncope.
- Family history of sudden cardiac death.
- Known structural heart disease.
- Abnormal ECG.
📌 Key learning points
- Tilt table testing classifies reflex syncope by heart rate and blood pressure response.
- Type 2B is cardioinhibitory syncope with asystole and is the group most likely to raise pacing discussions.
- Type 3 is vasodepressor syncope, where hypotension dominates and pacing is usually not helpful.
- NICE recommends selective rather than routine tilt testing in suspected vasovagal syncope.
- Always exclude high-risk cardiac causes before labelling recurrent blackouts as benign reflex syncope.
📚 References
- NICE Clinical Guideline CG109: Transient loss of consciousness in over 16s.
- European Society of Cardiology: Guidelines for the diagnosis and management of syncope.
