
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatony and Physiology of the Nephron
Related Subjects: |AP of the Thyroid |AP of the Parathyroid |AP of the Pituitary |AP of the Pancreas |AP of the Adrenal Gland |AP of the Oesophagus |AP of the Diaphragm |AP of the Large Bowel (Colon, Rectum, Anal Canal) |AP of Small Bowel |AP of the Biliary system |AP of the Bone Marrow |AP of the Eye |AP of the Pharynx |AP of the Larynx |AP of the Ear |AP of the Nose |AP of Male Genitalia |AP of the Breast |AP of the Stomach |AP of the Rectum |AP of the Spleen |AP of the Liver |AP of the Nephron
🩺 Nephron
Each kidney contains ~1 million nephrons, and together they regulate water, electrolytes, acid–base balance, and waste excretion. The nephron is not a passive filter but a dynamic filtration–reabsorption–secretion system under hormonal and neural control. Small changes in tubular transport produce major systemic effects, explaining why nephron physiology underpins hypertension, AKI, CKD, and drug responses. Always think: which segment is failing?
🧬 Structural Overview
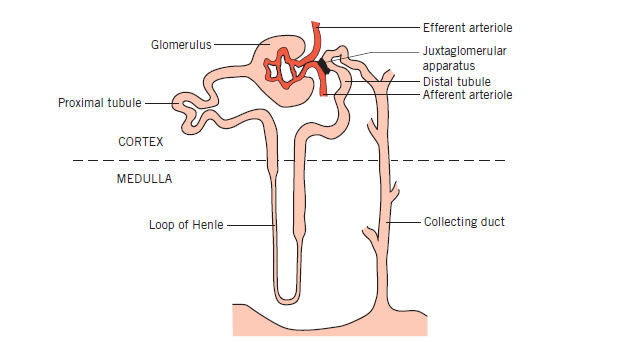
A nephron consists of a renal corpuscle (glomerulus + Bowman’s capsule) and a tubular system: proximal tubule → loop of Henle → distal tubule → collecting duct. Nephrons are arranged across cortex and medulla, allowing separation of filtration, bulk reabsorption, and fine regulation.
- Cortical nephrons: Short loops; major role in filtration and reabsorption.
- Juxtamedullary nephrons: Long loops; essential for urine concentration.
Juxtamedullary nephrons and the vasa recta are the anatomical basis of the kidney’s concentrating ability.
🩸 Renal Corpuscle: Glomerulus + Bowman’s Capsule
Blood enters the glomerulus via the afferent arteriole and exits via the efferent arteriole. Filtration is driven by hydrostatic pressure and regulated by arteriolar tone. The filtration barrier is size- and charge-selective, preventing protein loss.
🔬 Filtration Barrier
- Fenestrated endothelium (blocks cells)
- Glomerular basement membrane (negatively charged)
- Podocyte slit diaphragms
- ~180 L/day ultrafiltrate formed
- Normally protein-free
⚠️ Damage here → proteinuria, haematuria, nephrotic/nephritic syndromes. Efferent constriction ↑ GFR short-term but risks downstream ischaemia (ACE inhibitors effect).
🔄 Proximal Convoluted Tubule (PCT)
The PCT is the workhorse of the nephron, reabsorbing ~65–70% of filtered load. Transport is driven by basolateral Na⁺/K⁺ ATPase, making reabsorption largely iso-osmotic. Most nutrients and bicarbonate are reclaimed here.
- Na⁺, H₂O: ~65–70%
- Glucose, amino acids: ~100% (until saturated)
- HCO₃⁻: ~90%
- Phosphate, urate, drugs (organic acids/bases)
Clinical links:
- SGLT2 inhibitors → glycosuria + osmotic diuresis
- Fanconi syndrome → PCT failure (glycosuria, aminoaciduria, acidosis)
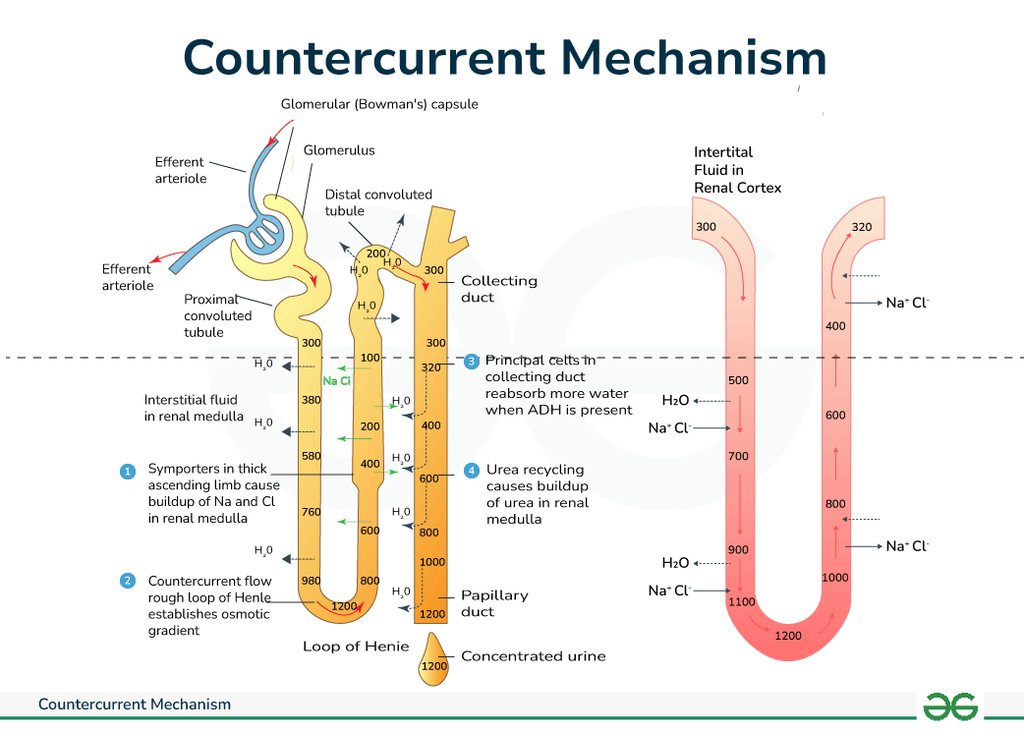
❄️ Loop of Henle
The loop of Henle generates the corticomedullary gradient via countercurrent multiplication. This gradient allows ADH-dependent water reabsorption later in the collecting duct.
Segments
- Descending limb: Water-permeable, solute-impermeable
- Ascending limb (TAL): Na⁺/K⁺/Cl⁻ reabsorption, water-impermeable
- Creates hypertonic medulla
- Dilutes tubular fluid
Loop diuretics (furosemide) block NKCC2 → collapse gradient → powerful diuresis + hypokalaemia.
⚙️ Distal Convoluted Tubule (DCT)
The DCT is a regulatory segment that fine-tunes electrolyte balance, especially calcium and sodium. Transport here is hormone-sensitive and less about volume than precision.
- Na⁺/Cl⁻ reabsorption (NCC transporter)
- Ca²⁺ reabsorption (PTH-dependent)
- Mg²⁺ handling
Thiazides act here → ↓ Na⁺ reabsorption + ↑ Ca²⁺ retention (useful in renal stones, risk of hypercalcaemia).
🚰 Collecting Duct System
The collecting duct determines final urine composition and is under strong hormonal control. It contains principal cells and intercalated cells.
Principal Cells
- Na⁺ reabsorption (ENaC)
- K⁺ secretion
- Water reabsorption (ADH → aquaporins)
Intercalated Cells
- α-cells: H⁺ secretion (acidosis defence)
- β-cells: HCO₃⁻ secretion (alkalosis defence)
Hormonal control:
- ADH → concentrates urine
- Aldosterone → Na⁺ retention, K⁺ loss
- ANP → natriuresis
📡 Juxtaglomerular Apparatus (JGA)
The JGA links tubular flow to glomerular filtration and systemic blood pressure.
- Macula densa: Senses distal NaCl
- JG cells: Release renin
- Mesangial cells: Structural support
Low NaCl → renin → RAAS activation → ↑ BP, ↑ GFR support.
⚙️ Integrated Nephron Physiology
- Filtration: Determines solute delivery (GFR).
- Bulk reabsorption: PCT + loop reclaim most filtrate.
- Fine regulation: DCT + collecting duct adjust final balance.
- Acid–base: H⁺ secretion + HCO₃⁻ handling.
- Volume control: RAAS, ADH, ANP coordinate response.
Renal function = interaction of haemodynamics + tubular transport + hormones. Failure in any one domain produces predictable biochemical patterns.
💊 Nephron Segments and Drug Targets
| Segment | Main Transport | Drug Example | Key Effect |
|---|---|---|---|
| PCT | Na⁺/H⁺, glucose | SGLT2 inhibitors | Glycosuria, mild diuresis |
| TAL | Na⁺/K⁺/Cl⁻ | Loop diuretics | Powerful diuresis |
| DCT | Na⁺/Cl⁻, Ca²⁺ | Thiazides | ↓ Ca²⁺ excretion |
| Collecting duct | ENaC, ADH | Amiloride, Desmopressin | K⁺-sparing, water control |
🧠 Clinical Integration
- Pre-renal AKI: ↓ perfusion → intact tubules → high Na⁺ reabsorption.
- ATN: PCT/TAL injury → Na⁺ wasting, muddy casts.
- Diabetes insipidus: ADH failure/resistance → dilute urine.
- RTA: Tubular acid-handling defects.
- CKD: Progressive nephron loss → hyperphosphataemia, acidosis, anaemia.
🩺 Clinical Pearl
When interpreting renal bloods, always localise the problem: Glomerulus (filtration), PCT/Loop (bulk handling), or DCT/Collecting duct (fine regulation). This transforms physiology into a practical diagnostic framework.
📌 Conclusion
The nephron is a precisely organised functional unit in which structure dictates physiology. Filtration occurs at the corpuscle, bulk reabsorption in the PCT and loop, and final control in the distal nephron. Hormonal integration and countercurrent mechanisms allow humans to survive wide variations in intake and illness. Mastery of nephron physiology is essential for understanding fluid balance, electrolyte disorders, and renal pharmacology.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery