
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Tuberculosis
Related Subjects: |Assessing Breathlessness |Fever - Pyrexia of unknown origin |Tuberculosis |TB Meningitis |Miliary Tuberculosis |Lady Windermere syndrome
🌍 Tuberculosis (TB) remains a major global infectious disease and an important UK public health diagnosis. 🧪 Offer HIV testing to people with suspected or confirmed TB, and consider other immunosuppression risks such as transplant medicines, biological therapy, corticosteroids, diabetes, CKD and malnutrition. 💉 BCG mainly protects children against severe disseminated TB, especially TB meningitis and miliary TB; it is much less reliable at preventing adult pulmonary TB. 📋 All suspected or confirmed active TB is notifiable in the UK, regardless of site of disease.
🔬 Microbiology
- Mycobacterium tuberculosis is an obligate aerobe, acid-fast bacillus. On Ziehl–Neelsen staining it appears as 🔴 red rods.
- Its lipid-rich cell wall contains mycolic acids, which explain acid-fastness, resistance to drying, slow growth and survival inside macrophages.
- ⏱️ It is slow-growing, with a generation time of roughly 12–18 hours, so culture may take weeks.
- 🧪 Cord factor is associated with virulence, granuloma formation and inhibition of normal macrophage killing.
- Classically, M. tuberculosis is niacin positive and nitrate reduction positive, although modern practice relies heavily on NAAT, culture and drug susceptibility testing.
🧠 Pathophysiology: why TB behaves like this
- After inhalation, bacilli reach the alveoli and are taken up by macrophages. The organism can survive intracellularly, so the immune system responds with a delayed type IV hypersensitivity reaction.
- Activated T cells and macrophages form granulomas, which attempt to wall off infection. This explains caseating granulomas, latent infection and later reactivation.
- Reactivation tends to affect the upper lobes because M. tuberculosis favours high oxygen tension.
- Severe immunosuppression may prevent good granuloma formation, so TB may be disseminated, smear-negative or radiologically atypical.
🌍 Epidemiology & Risk: UK focus
- UK risk is higher with recent close contact, birth or prolonged residence in a high-incidence country, homelessness, imprisonment, alcohol or drug misuse, previous untreated TB, and immunosuppression.
- 📈 HIV increases the risk of both reactivation and extrapulmonary TB. In advanced HIV, chest imaging may be non-classical or even deceptively normal.
- 💊 MDR-TB means resistance to at least isoniazid and rifampicin. RR-TB means rifampicin-resistant TB. These require specialist TB services.
- 🏥 Always consider TB in a patient with constitutional symptoms, prolonged cough, abnormal CXR, lymphadenopathy, sterile pyuria, meningitis of subacute onset, or unexplained pericardial/pleural effusion.
🫁 Clinical Types
- Primary TB: initial infection, often asymptomatic. A Ghon focus plus involved hilar lymph nodes forms a Ghon complex.
- Latent TB infection: immune containment of infection. The patient has no symptoms, no radiological evidence of active disease and is not infectious, but immunological tests may be positive.
- Post-primary / reactivation TB: classically apical pulmonary disease with cavitation, cough, haemoptysis, fever, night sweats and weight loss.
- Miliary TB: haematogenous dissemination causing diffuse “millet seed” lesions 🌾 and systemic illness.
- Extrapulmonary TB:
- 🧠 CNS: TB meningitis, tuberculoma, spinal TB / Pott disease.
- 🚻 Genitourinary: sterile pyuria, epididymo-orchitis, infertility.
- 🍽️ Gastrointestinal: ileocaecal disease, abdominal pain, obstruction, ascites.
- ❤️ Pericardial: pericarditis, effusion, later constrictive pericarditis.
- 🧂 Adrenal: adrenal destruction causing primary adrenal insufficiency.
- 🦴 Bone/joint: vertebral collapse, chronic monoarthritis, cold abscess.
- 🧬 Lymph node TB: classically chronic painless cervical lymphadenopathy.
📋 Clinical Features
- 🗣️ Persistent cough, especially if lasting more than 3 weeks, with or without sputum or haemoptysis.
- 🌡️ Fever, night sweats, anorexia, weight loss and fatigue.
- 😮 Chest pain or breathlessness, especially with pleural or pericardial involvement.
- ⚠️ Extrapulmonary clues include meningism, confusion, back pain, spinal deformity, sterile pyuria, lymphadenopathy, ascites, monoarthritis or adrenal insufficiency.
- 👶 In children, TB can be non-specific: poor growth, fever, lethargy, cough, lymphadenopathy or contact with an infectious adult.
🚨 Infection Control & Public Health
- 📋 Notify suspected or confirmed active TB promptly through the local TB/public health pathway.
- 😷 Suspected infectious pulmonary or laryngeal TB should be managed with appropriate respiratory isolation while being assessed.
- 🏠 Contact tracing is coordinated by specialist TB services and public health teams. Household contacts, children and immunosuppressed contacts are particularly important.
- 🧪 Infectiousness is highest with smear-positive pulmonary or laryngeal TB, cavitating disease, cough and aerosol-generating exposures.
🔎 Investigations: UK/NICE-style approach
- 🩻 Chest X-ray is the usual initial imaging test for suspected pulmonary TB. CT may help define complex disease, lymph nodes, cavitation or alternative diagnoses.
- 🧪 Sputum testing: send sputum, induced sputum or BAL for AFB smear, culture and NAAT. NAAT can rapidly identify M. tuberculosis and may detect rifampicin resistance.
- 🧫 Culture remains the reference standard because it confirms the organism and enables full drug susceptibility testing.
- 🧬 IGRA/TST: mainly used for latent TB assessment and contact screening. IGRA is not affected by previous BCG, but neither IGRA nor TST reliably distinguishes active from latent TB.
- 🔬 Extrapulmonary TB: obtain tissue or fluid where possible for microscopy, culture, NAAT and histology. Histology may show caseating granulomas, but microbiological confirmation is preferred.
- 🧠 Suspected CNS TB: urgent neuroimaging if indicated, lumbar puncture where safe, CSF microscopy/culture/NAAT, and early specialist treatment because delay worsens outcome.
- 🧪 Baseline tests before treatment: LFTs, U&Es, FBC, HIV test, hepatitis B/C where relevant, pregnancy status where appropriate, and visual acuity/colour vision if ethambutol is used.
💊 Management: Drug-Sensitive Active TB
- Standard 6-month regimen for most drug-sensitive pulmonary TB:
- Initial phase, 2 months: isoniazid + rifampicin + pyrazinamide + ethambutol = HRZE.
- Continuation phase, 4 months: isoniazid + rifampicin = HR.
- 💊 Give pyridoxine with isoniazid when there is increased neuropathy risk, such as pregnancy, diabetes, HIV, alcohol dependence, malnutrition, renal disease or existing neuropathy.
- 🧠 CNS TB usually requires longer treatment, commonly around 12 months, under specialist guidance.
- 🦴 Bone/joint TB, disseminated TB, drug-resistant TB or interruptions in treatment may also need longer or modified treatment.
- 🤝 Adherence support is essential. Use enhanced case management for people at risk of poor adherence. DOT is not for everyone, but is useful where adherence risk is high.
- 💉 Adjunct corticosteroids are important in TB meningitis and are often used in TB pericarditis, guided by specialists.
🧫 Key principles of TB treatment: Never start just one anti-TB drug, and never add just one drug to a failing regimen. TB treatment requires combination therapy to prevent resistance, relapse and treatment failure. Suspected or confirmed MDR-TB, treatment failure, significant drug toxicity, HIV co-infection, pregnancy, CNS TB, disseminated TB or complex extrapulmonary TB should be managed with specialist TB, respiratory, infectious diseases and microbiology input.
💊 Core Treatment Principles
- Use combination therapy treat with RIPE: rifampicin, isoniazid, pyrazinamide and ethambutol initially.
- Check drug susceptibility — culture and sensitivity results and see if resistance is present.
- Do not use monotherapy — single-drug exposure rapidly selects resistant Mycobacterium tuberculosis.
- Do not add one drug to a failing regimen — can cause rapid resistance if the existing regimen is already ineffective.
- Assess adherence carefully — poor adherence is a major cause of treatment failure, relapse and resistance.
- Consider directly observed therapy for high-risk patients, previous non-adherence, homelessness, substance misuse, MDR-TB or recurrent TB.
- Screen for HIV and comorbidities — HIV, diabetes, renal disease, liver disease, alcohol misuse and immunosuppression affect outcomes and treatment choices.
- Monitor toxicity — check baseline and follow-up liver function, renal function, vision with ethambutol, neuropathy risk and drug interactions.
- Give pyridoxine when indicated — vitamin B6 reduces isoniazid-related peripheral neuropathy, especially in pregnancy, malnutrition, diabetes, HIV, renal failure or alcohol dependence.
- Notify TB cases — TB is a notifiable disease and contact tracing is essential for public health control.
⚠️ When to Seek Specialist Advice
- Suspected or confirmed MDR-TB or rifampicin resistance
- Treatment failure, relapse or previous incomplete TB treatment
- CNS TB, miliary TB, spinal TB or pericardial TB
- Pregnancy, breastfeeding or paediatric TB
- HIV co-infection or significant immunosuppression
- Severe liver disease, renal failure or major drug interactions
- Significant adverse effects from TB medication
💊 High-Yield Drug Toxicities
- 💊 Isoniazid → hepatitis, peripheral neuropathy, seizures in overdose. Prevent neuropathy with pyridoxine when risk is increased.
- 🟠 Rifampicin → hepatitis, orange urine/tears, thrombocytopenia, and potent enzyme induction causing major drug interactions.
- 🔥 Pyrazinamide → hepatitis, hyperuricaemia and gout.
- 👁️ Ethambutol → optic neuritis with reduced visual acuity and red-green colour impairment.
- 👂 Aminoglycosides, now mainly in selected drug-resistant TB contexts, can cause ototoxicity and nephrotoxicity.
- 🧬 Linezolid, used in some drug-resistant TB regimens, can cause myelosuppression, peripheral neuropathy and optic neuropathy.
🤝 TB & HIV
- 🧪 Offer HIV testing to all people with suspected or confirmed TB.
- 📷 TB in advanced HIV may be extrapulmonary, disseminated, smear-negative or radiologically atypical.
- 💊 ART timing is specialist-led. In general, people with CD4 <50 cells/µL usually start ART within about 2 weeks of starting TB treatment once stable and tolerating therapy. Others often start within 8–12 weeks.
- 🧠 Avoid very early ART in CNS TB unless specialist advice supports it, because immune reconstitution may worsen intracranial inflammation.
- ⚠️ Rifampicin has major interactions with ART, anticoagulants, antiepileptics, steroids, contraception and many other drugs. Always check interactions and involve TB/HIV specialists.
💤 Latent TB Infection
- Latent TB means the immune system has contained infection: the patient is asymptomatic, not infectious and has no evidence of active disease.
- 🧪 Testing is usually with IGRA and/or TST depending on age, risk and local pathway.
- 🚫 Before treating latent TB, exclude active TB clinically and radiologically; monotherapy or incomplete therapy in active disease risks resistance.
- 💊 Latent TB treatment options include rifampicin/isoniazid-based regimens depending on age, risk, interactions and specialist/local policy.
- 🧪 Check baseline risk factors for hepatotoxicity and relevant viral hepatitis testing before treatment where indicated.
💉 BCG Vaccination
- BCG is not routinely given to all children in the UK; it is targeted to babies, children or adults at higher risk of TB exposure.
- It is most useful for preventing severe childhood TB, particularly TB meningitis and miliary TB.
- BCG can affect TST results but does not affect IGRA results.
🆕 Newer TB drugs and MDR/RR-TB
Modern drug-resistant TB regimens are increasingly all-oral and specialist-led. They may include bedaquiline, delamanid, pretomanid, linezolid and fluoroquinolones such as moxifloxacin. Bedaquiline, delamanid and moxifloxacin can prolong the QT interval, so ECG monitoring is important. Linezolid can cause myelosuppression, peripheral neuropathy and optic neuropathy. These regimens can shorten treatment and avoid injectable toxicity, but they require TB specialist oversight, drug susceptibility results and careful monitoring.
🧠 Exam Pearls
- 🔴 Acid-fast bacillus + chronic cough/night sweats/weight loss = think TB.
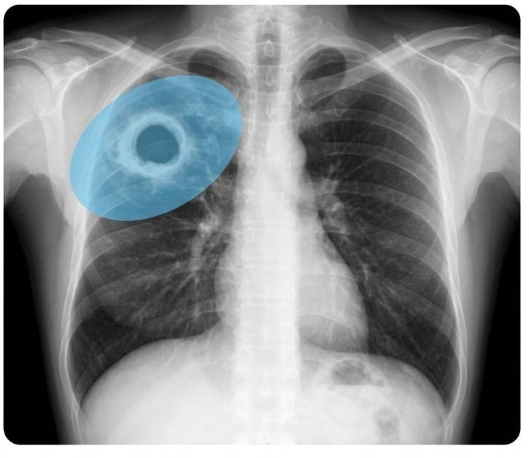
- 🩻 Upper-lobe cavitation suggests reactivation TB.
- 🌾 Diffuse tiny nodules = miliary TB.
- 🧪 IGRA/TST support latent TB diagnosis but do not prove active TB.
- 🧫 Culture is slow but remains vital for confirmation and susceptibility testing.
- 👁️ Ethambutol = optic neuritis; 🟠 rifampicin = orange secretions and enzyme induction; 💊 isoniazid = neuropathy/hepatitis; 🔥 pyrazinamide = gout/hepatitis.
- 📋 Active TB is notifiable in the UK.
⚠️ Clinical safety point: suspected TB should not be managed in isolation by a non-specialist. Involve respiratory/infectious diseases/TB specialist teams early, notify public health pathways, assess infectiousness, and consider contact tracing, adherence support and drug interactions from the start.
TB cavity
Miliary TB

| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery