
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Alzheimer disease (Dementia) ✅
Related Subjects: |Behavioural and Psychological (BPSD) Symptoms of Dementia |Alzheimer disease (Dementia)
🧠 Alzheimer’s disease is the most common cause of dementia. It causes a gradual, progressive decline in memory, thinking, language, behaviour and daily function. Diagnosis is clinical, supported by collateral history, cognitive testing, examination and investigations to exclude reversible or alternative causes.
ℹ️ About
- Alzheimer’s disease usually presents insidiously with progressive short-term memory loss, impaired learning, word-finding difficulty and reduced ability to manage daily activities.
- Collateral history from a family member or carer is essential, as patients may lack insight into functional decline.
- Progression is typically gradual, unlike vascular dementia, which may show a stepwise decline.
- Delirium, depression, medicines, alcohol, sensory impairment and metabolic disturbance can mimic or worsen cognitive symptoms.
🧬 Pathophysiology
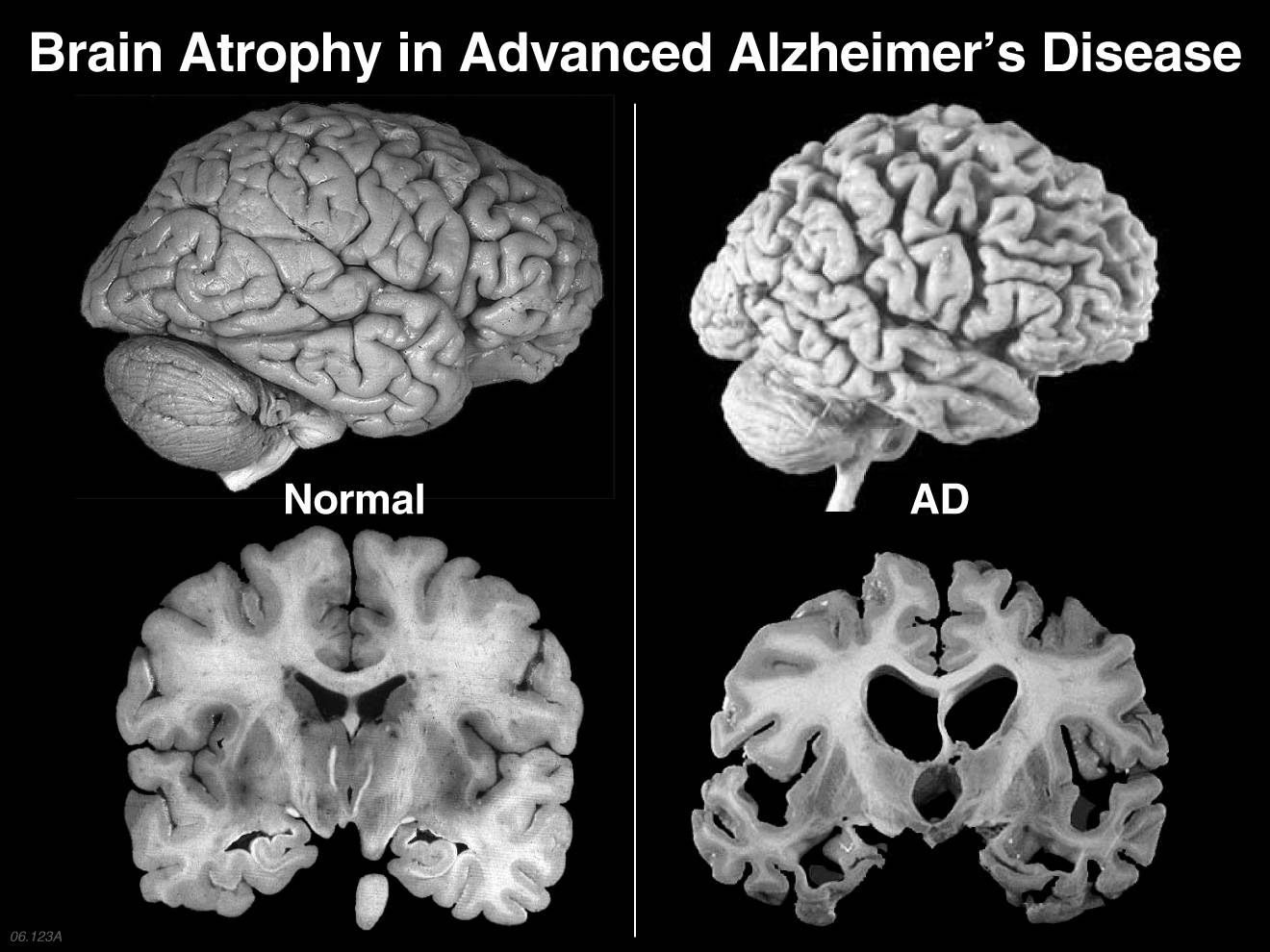
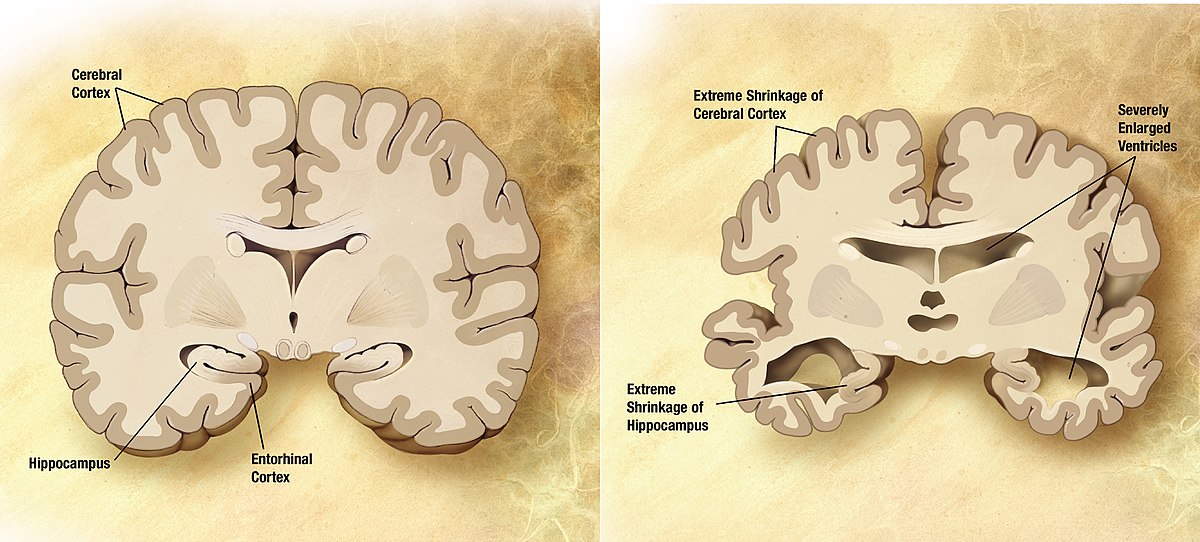
- Alzheimer’s disease is associated with synaptic failure, neuronal loss and cerebral atrophy, especially in the hippocampus and medial temporal lobes.
- β-amyloid plaques are extracellular deposits that disrupt neuronal signalling and trigger inflammation.
- Neurofibrillary tangles are intracellular aggregates of hyperphosphorylated tau protein and correlate with disease severity.
- Loss of cholinergic neurons contributes to problems with memory and attention, which is why acetylcholinesterase inhibitors can provide symptomatic benefit.
- Most cases are sporadic; rare familial forms are linked to mutations such as APP, PSEN1 and PSEN2. ApoE ε4 increases risk but is not used as a routine diagnostic test.
⚠️ Risk Factors
- Increasing age is the strongest risk factor; Alzheimer’s disease becomes much more common in later life.
- Family history increases risk, especially if there is early-onset dementia in a first-degree relative.
- Genetics: ApoE ε4 increases susceptibility, while rare mutations such as APP, PSEN1 and PSEN2 can cause familial early-onset Alzheimer’s disease.
- Cardiovascular risk factors such as hypertension, diabetes, smoking, obesity and hyperlipidaemia are associated with increased dementia risk.
- Previous head injury, especially repeated traumatic brain injury, may increase risk.
- Lower cognitive reserve, social isolation, physical inactivity, hearing loss and depression are associated with higher dementia risk.
- Alcohol excess and poor sleep may contribute to cognitive decline and should be addressed as part of prevention and assessment.
💡 Clinical Pearl: Risk factors are not diagnostic. In practice, they help identify people who may benefit from prevention advice, medication review, vascular risk optimisation and earlier assessment if symptoms develop.
🔎 Assessment
- Take a history from the patient and an informant, focusing on onset, progression, memory, language, visuospatial skills, behaviour, mood, medicines, alcohol and activities of daily living.
- Use a structured cognitive tool such as MoCA, MMSE, 6CIT or ACE-III, but do not rely on a score alone.
- Assess function, falls risk, driving, safeguarding, capacity, carer strain and home safety.
- Screen for depression and delirium, especially if symptoms are fluctuating or sudden in onset.
🧪 Investigations
- Blood tests commonly include FBC, U&Es, LFTs, calcium, glucose/HbA1c, TFTs, B12 and folate.
- Consider urine testing, infection screen or other tests if clinically indicated.
- Medication review is important: anticholinergics, sedatives, opioids, benzodiazepines and alcohol may worsen cognition.
- Structural imaging with CT or MRI can help exclude tumour, subdural haematoma, normal-pressure hydrocephalus or significant vascular disease.
- Specialist services may use MRI patterns, FDG-PET, amyloid imaging or CSF biomarkers where diagnosis remains uncertain.
🖥️ Imaging Features
- MRI: medial temporal and hippocampal atrophy support Alzheimer’s disease.
- CT: may show cerebral atrophy and helps exclude other structural pathology.
- Vascular changes: prominent small-vessel disease or infarcts may suggest vascular or mixed dementia.
- Imaging supports the diagnosis but does not replace clinical assessment.
👩⚕️ Behavioural and Psychological Symptoms
- Symptoms may include anxiety, depression, apathy, agitation, sleep disturbance, wandering, hallucinations, delusions or aggression.
- Look for triggers: pain, constipation, urinary retention, infection, dehydration, hunger, overstimulation, sleep disruption or environmental change.
- Use non-drug strategies first: reassurance, routine, orientation cues, calm communication, activity, sleep hygiene and carer support.
- Antipsychotics should only be considered if the person is severely distressed or there is risk of harm, and after discussing risks and benefits.
- Avoid antipsychotics where possible in dementia with Lewy bodies or Parkinson’s disease dementia because of severe sensitivity reactions.
💊 NICE-Compatible Drug Treatment
| Treatment | When to Consider | Key Points |
|---|---|---|
| Donepezil
Rivastigmine Galantamine |
Mild-to-moderate Alzheimer’s disease | Acetylcholinesterase inhibitors. Choice should consider adverse effects, adherence, comorbidities, interactions and formulation preference. Monitor pulse, weight, GI effects, sleep disturbance and syncope risk. |
| Memantine | Moderate Alzheimer’s disease if AChE inhibitors are not tolerated or contraindicated; severe Alzheimer’s disease | NMDA receptor antagonist. Monitor for dizziness, headache, constipation, confusion and renal function where relevant. |
| Memantine added to an AChE inhibitor | Consider in moderate Alzheimer’s disease; offer in severe Alzheimer’s disease if already taking an AChE inhibitor | Do not stop an AChE inhibitor solely because dementia has become severe. Review benefit, adverse effects and goals of care. |
| Antidepressants | Clinically significant depression or anxiety | Use after assessment for reversible causes and psychosocial triggers. Monitor falls risk, hyponatraemia, bleeding risk and QT interval where relevant. |
| Antipsychotics | Severe distress, psychosis, aggression or risk of harm after non-drug approaches have failed | Use the lowest effective dose for the shortest possible time. Discuss stroke, sedation, falls, extrapyramidal effects and mortality risk. Review frequently. |
| Benzodiazepines | Rarely, for short-term crisis use only | High risk of sedation, falls, confusion and paradoxical agitation. Avoid routine use in frail older adults. |
🏡 Non-Drug Management
- Offer cognitive stimulation therapy for people with mild-to-moderate dementia where available.
- Encourage physical activity, social engagement, good sleep, hearing and vision optimisation, nutrition and hydration.
- Support carers with education, respite planning, crisis contacts and assessment of carer strain.
- Review driving, work, finances, lasting power of attorney and advance care planning early while the person has capacity.
- Optimise vascular risk factors such as hypertension, diabetes, smoking and hyperlipidaemia, especially where mixed dementia is possible.
⚠️ Complications
- Falls, fractures, wandering, malnutrition, dehydration and medication errors.
- Delirium triggered by infection, constipation, pain, dehydration or hospital admission.
- Swallowing difficulty, aspiration pneumonia, pressure ulcers and immobility in advanced disease.
- Carer burnout, safeguarding concerns and loss of independence.
🌅 Advanced Disease and End-of-Life Care
- Focus on comfort, dignity, nutrition, hydration, pressure care, mouth care and symptom control.
- Discuss ceilings of care, hospital transfer, resuscitation status and preferred place of care early and sensitively.
- Support families and carers, as dementia is a long illness with major emotional and practical burden.
💡 Exam Pearl: Alzheimer’s disease usually causes gradual progressive memory impairment with hippocampal or medial temporal atrophy. Stepwise decline suggests vascular dementia; prominent early hallucinations, fluctuating cognition and parkinsonism suggest dementia with Lewy bodies.
📚 NICE Guidance
- NICE NG97: Dementia: assessment, management and support for people living with dementia and their carers.
- NICE TA217: Donepezil, galantamine, rivastigmine and memantine for the treatment of Alzheimer’s disease.
- NICE QS184: Dementia quality standard.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery