Related Subjects:
|Fractured Neck of Femur
|Fractured Shaft Femur
|Supracondylar Femur Fractures
|Supracondylar Humerus Fractures
|Femoral fractures
|Fractured Tibia and Fibula
|Pelvic fractures
Clavicle Fractures 🦴 are very common - especially in children and young adults after sports or falls, and in the elderly with osteoporosis.
👉 Most heal well with conservative management. There is no proven long-term functional benefit to surgical fixation in most cases.
🚨 Surgery is reserved for specific indications (open fracture, neurovascular compromise, severe displacement).
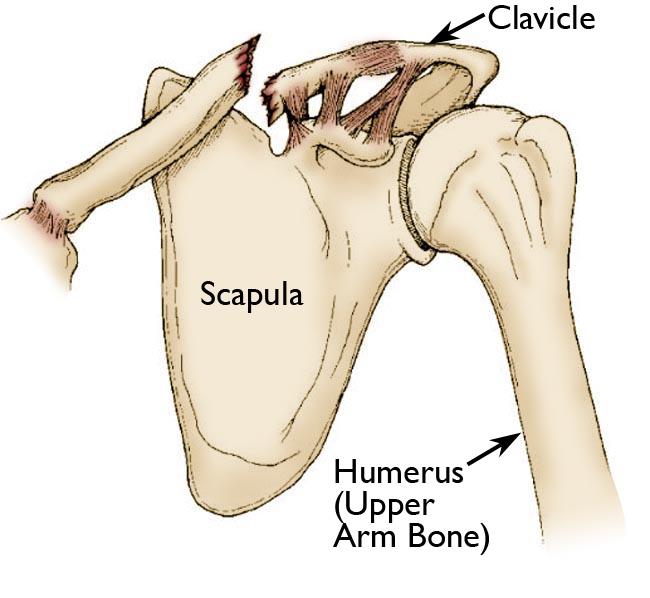
📖 About
- Most frequently fractured bone in childhood 👶.
- High-energy sports injuries, FOOSH, or low-impact falls in elderly.
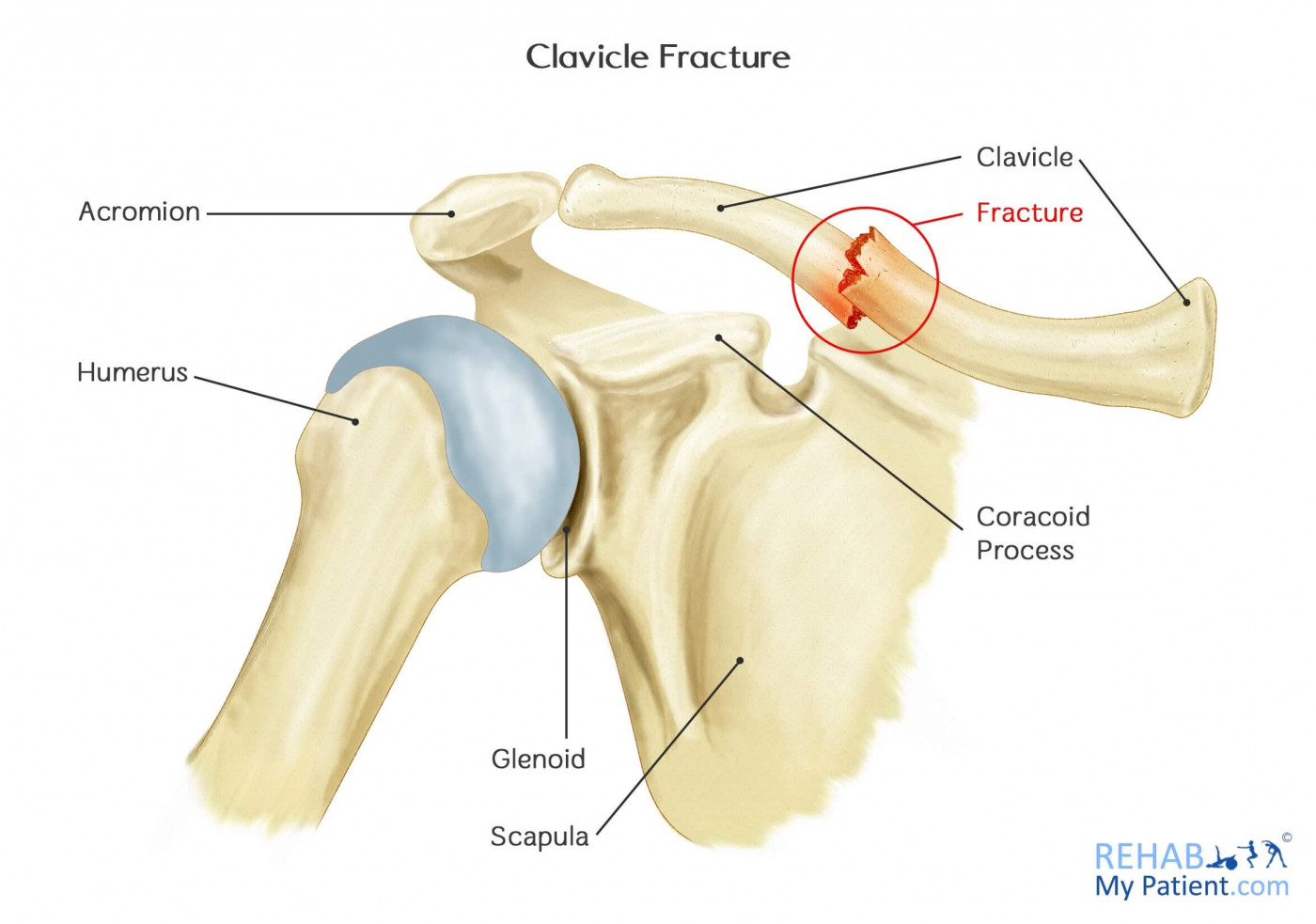
- Up to 80% involve the middle third of the clavicle.
⚙️ Aetiology
- Fall on an outstretched hand (FOOSH) ✋.
- Direct blow to clavicle (contact sports, road traffic accidents 🚲).
- Indirect trauma via shoulder girdle.
📊 Allman Classification
- Type I (≈80%): Middle third - most common; usually stable.
- Type II (≈15%): Lateral third - often unstable; higher risk of nonunion.
- Type III (≈5%): Medial third - rare, often from major trauma; may involve great vessels or chest injuries.
🔎 Alternative (Neer)
- Further subcategorises lateral third fractures by coracoclavicular ligament involvement → predicts stability and nonunion risk.
🩺 Clinical Features
- Sharp pain over clavicle/shoulder.
- Swelling or deformity over clavicle or anterior chest wall.
- Crepitus/step deformity on palpation.
- Reduced shoulder movement due to pain.
- Systemic response: dizziness, nausea, blurred vision (pain-related).
- Always check for:
- Skin tenting / open wound
- Neurovascular compromise (brachial plexus, subclavian vessels)
- Pneumothorax / haemothorax if medial fracture
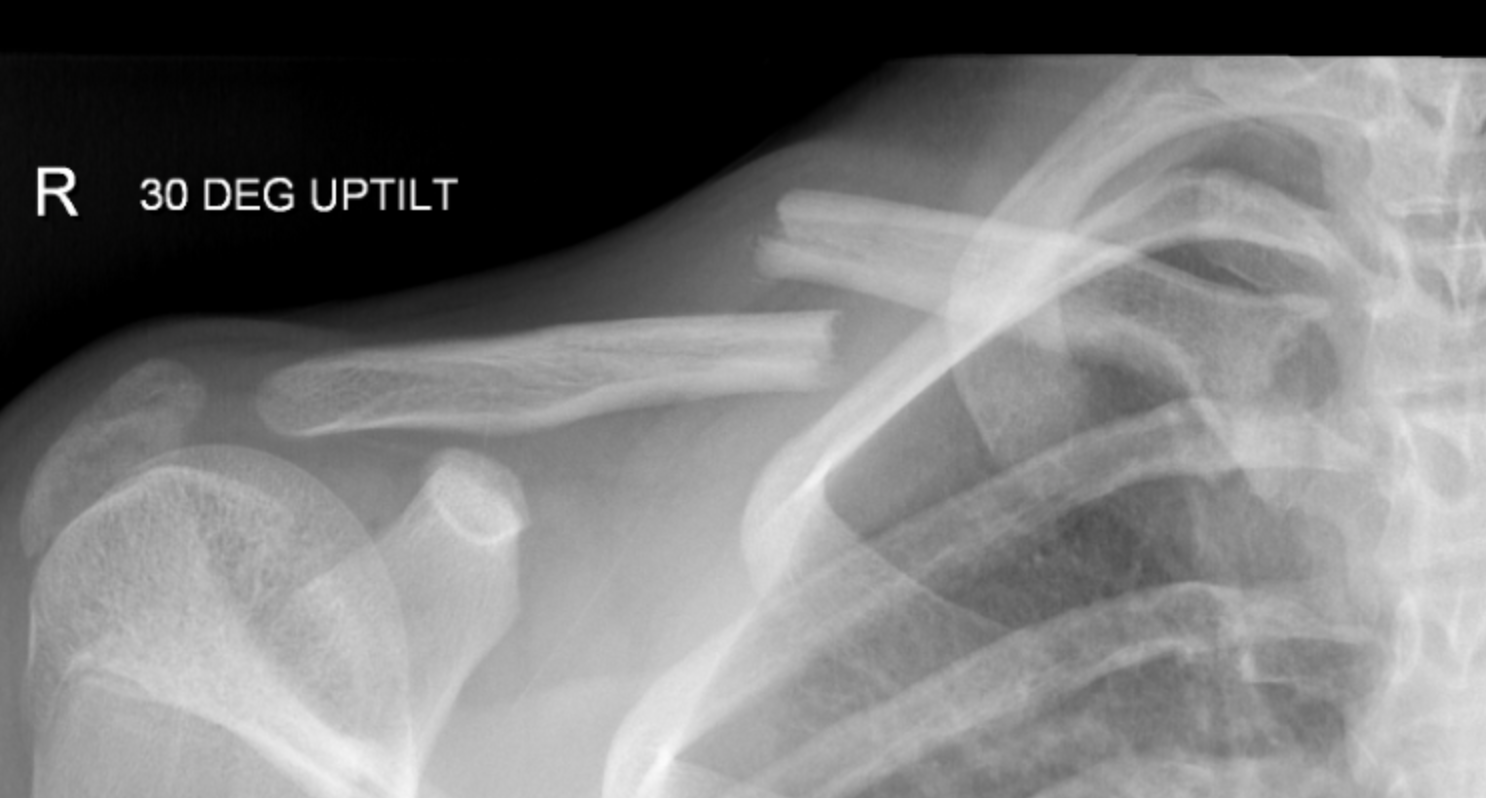
🧪 Investigations
- X-ray: AP clavicle ± 15° cephalic tilt view (best for fracture displacement).
- CT chest: Medial fractures with posterior displacement → exclude mediastinal injury.
- MRI/CT: Rarely, for complex or nonunion cases.
- Ultrasound: Radiation-free and useful in children.
⚠️ Complications
- Nonunion (esp. lateral fractures; risk up to 15%).
- Malunion - bony bump/cosmetic, usually asymptomatic.
- Neurovascular injury - brachial plexus, subclavian artery/vein (rare).
- Pneumothorax / Haemothorax - medial/posterior displacement.
- Infection - only if open or post-surgery.
💊 Management
- Initial: Analgesia, wound care, tetanus prophylaxis if open wound. Document neurovascular status.
- Conservative (majority):
- Broad-arm sling 2–3 weeks until pain allows mobilisation.
- Figure-of-eight brace no longer preferred (no proven benefit).
- Early physiotherapy for ROM once pain settles.
- Children: callus prominence common, remodels with time.
- Surgical Indications (≈5–10%):
- Open fracture or skin tenting (threatened skin) 🚨
- Neurovascular compromise
- Severely displaced/comminuted fracture with >2 cm shortening
- Unstable lateral third fractures (coracoclavicular ligament disruption)
- Symptomatic nonunion
📌 OSCE / Exam Pearls
- Always palpate along entire clavicle - ensure no second injury (esp. sternoclavicular joint).
- Lateral third fractures have highest nonunion risk → consider surgery earlier.
- In children, remodelling is excellent; reassure about cosmetic bumps.
- Check for neurovascular compromise (subclavian vessels, brachial plexus) in displaced medial injuries.
📚 References
- Rockwood & Green’s Fractures in Adults, 9th ed.
- British Orthopaedic Association (BOA) guidance on clavicle fractures.
- Robinson CM. Fractures of the clavicle in the adult. J Bone Joint Surg Br. 1998;80(3):476-484.
- NICE Clinical Knowledge Summaries (CKS): Clavicle fracture. 2023.
