Related Subjects:
|Herpes Varicella-Zoster (Shingles) Infection
|Chickenpox Varicella Infection
|Varicella Cerebral Vasculopathy
|Herpes Viruses
|Herpes Zoster Ophthalmicus (HZO) Shingles
|MonkeyPox
|Mumps
|Measles
|Rubella (German Measles)
|Epstein-Barr Virus infection
|Cytomegalovirus (CMV) infections
|CMV retinitis infections
|Toxoplasmosis
💡 Key Point: Lung transplantation is life-saving for end-stage lung disease but carries high risks of infection, rejection, and long-term complications due to lifelong immunosuppression.
📖 About
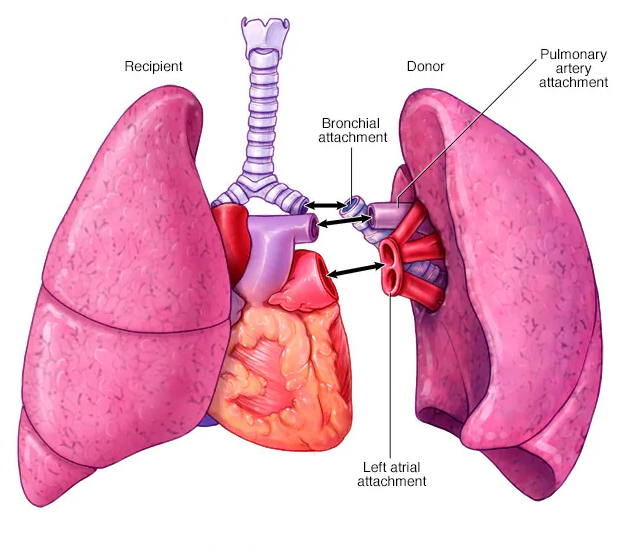
- Procedure involves replacing one or both diseased lungs with donor lungs.
- Performed as single or double lung transplants depending on the underlying condition.
- Generally offered to patients <60 years, though exceptions exist.
- Requires lifelong immunosuppression (Ciclosporin, Tacrolimus, Steroids, Mycophenolate, Azathioprine, anti-lymphocyte globulin).
- Immunosuppression ➝ 🚨 high risk of opportunistic infections.
🫁 Types
- Single Lung Transplant: Used in conditions with infection risk confined to one lung (e.g. COPD, IPF).
- Double Lung Transplant: Both lungs replaced (sequentially). Preferred in Cystic Fibrosis, IPF, Pulmonary Hypertension.
🎯 Indications
- Cystic Fibrosis (➡️ DOUBLE).
- Emphysema & Alpha-1 antitrypsin deficiency.
- Idiopathic Pulmonary Fibrosis.
- Advanced COPD.
- Connective tissue–related pulmonary fibrosis.
- Chronic Hypersensitivity Pneumonitis.
- Advanced Sarcoidosis.
- Primary Pulmonary Hypertension (➡️ DOUBLE).
- Rare diseases: Langerhans cell granulomatosis, Lymphangioleiomyomatosis.
⚠️ Complications
- Infections: CMV, Aspergillus, PJP; risk highest if donor seropositive & recipient seronegative.
- Acute Rejection: Weeks–months; managed by ↑ immunosuppression.
- Chronic Rejection: Bronchiolitis Obliterans Syndrome (BOS) ➝ progressive breathlessness & airflow limitation.
- Drug Toxicity: Calcineurin inhibitors ➝ nephrotoxicity & hypertension.
- Malignancy: Skin cancers & post-transplant lymphoproliferative disorder (PTLD).
- GI Side Effects: Nausea, diarrhoea, peptic ulcer disease.
🩺 Post-Transplant Care
- 📈 Monitor lung function (spirometry, imaging) for early rejection.
- 🔬 Screen for infections (CMV, PJP, Aspergillus).
- 💊 Prophylaxis: TMP-SMX (Bactrim) for PJP, antivirals if indicated.
- 🏃♂️ Pulmonary rehab for recovery & QoL.
- ⚖️ Regular drug-level monitoring to balance efficacy vs toxicity.
- 📢 Patient education: adherence, infection precautions, recognising rejection.
📊 Prognosis
- Median survival: 5–7 years, though some survive much longer.
- Better outcomes: Younger patients, double lung transplants, cystic fibrosis.
- Chronic rejection (BOS) ➝ leading cause of late mortality.
- Careful monitoring improves QoL and prolongs survival.
📚 References
3 Clinical Cases - Lung Transplantation 🫁🔄
- Case 1 - End-stage COPD 🚬: A 62-year-old man with GOLD stage 4 COPD, FEV₁ 22% predicted, on long-term oxygen therapy, presents with worsening breathlessness despite maximal inhaler therapy and pulmonary rehab. Multiple admissions in past year. Teaching: COPD is the commonest indication for lung transplant worldwide. Candidates are selected when prognosis is poor and quality of life severely impaired despite optimal treatment. Typically offered a single lung transplant if age/fitness appropriate.
- Case 2 - Idiopathic Pulmonary Fibrosis 🌫️: A 55-year-old woman with rapidly progressive IPF (FVC 38% predicted, DLCO 30%) is hypoxaemic at rest and desaturates with exertion. She is referred early for transplant assessment. Teaching: IPF carries the worst prognosis of the interstitial lung diseases. Double lung transplantation is usually performed, as single lung grafts are at higher risk of infection and poor long-term function.
- Case 3 - Cystic Fibrosis 🧬: A 28-year-old woman with CF and chronic Pseudomonas colonisation has severe bronchiectasis, FEV₁ 18% predicted, and recurrent haemoptysis requiring embolisation. She is cachectic despite nutritional support. Teaching: Bilateral lung transplantation is the only curative option in advanced CF. It removes the diseased lungs and associated reservoir of infection. Post-op care requires aggressive immunosuppression and infection prophylaxis.
