Related Subjects:
|Iron deficiency Anaemia
|Haemolytic anaemia
|Macrocytic anaemia
|Megaloblastic anaemia
|Microcytic anaemia
|Myelodysplasia
|Myelofibrosis
🩸 A typical patient with megaloblastic anaemia presents with:
Macrocytic anaemia + thrombocytopenia + ↓ reticulocyte count + ↑ LDH (marker of ineffective erythropoiesis).
📖 About
- Haemoglobin is low, with MCV > 96 fl.
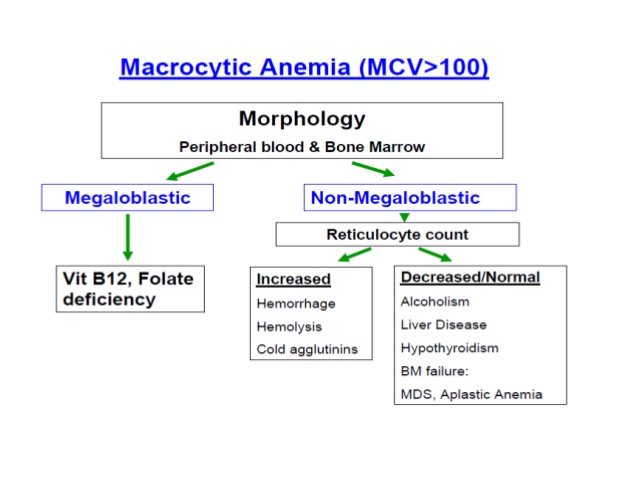
- Macrocytosis is the hallmark, but not all causes are megaloblastic.
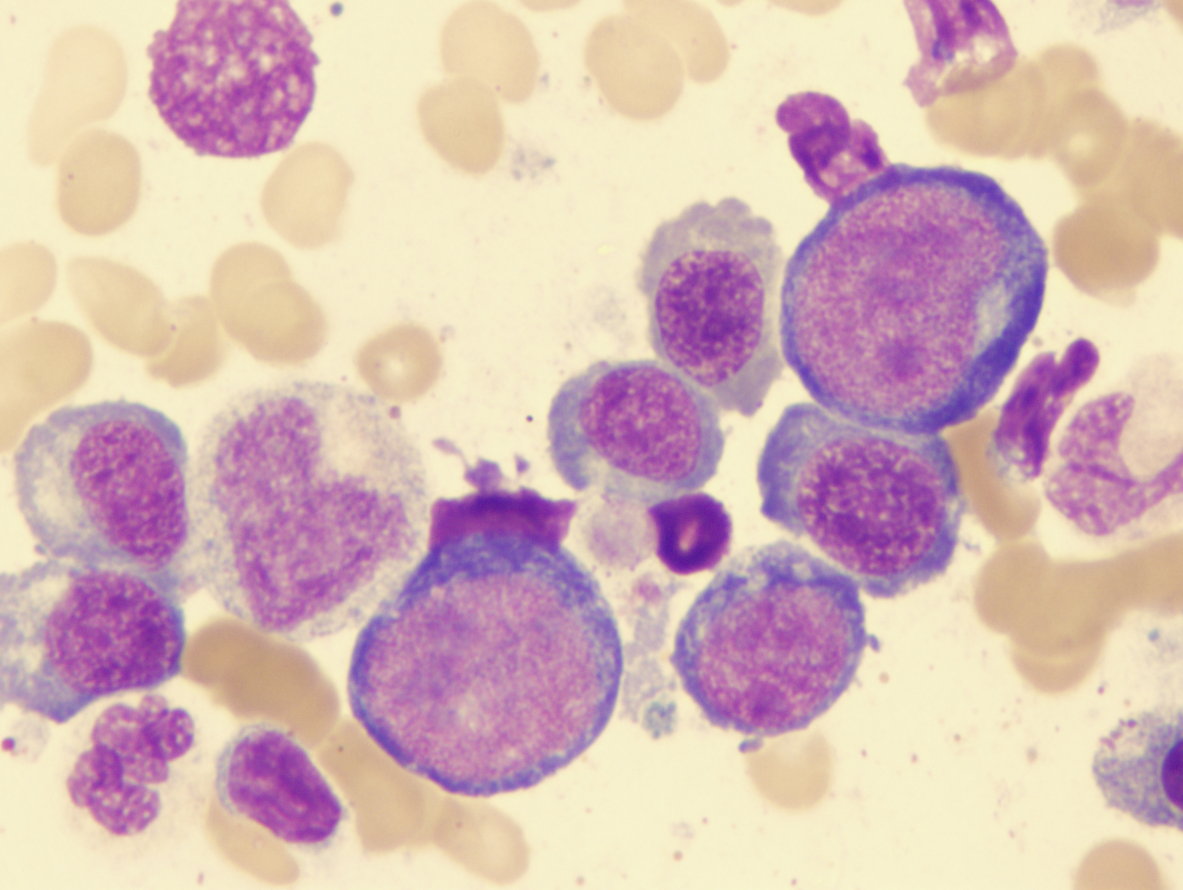
🔬 Megaloblasts
- Megaloblasts = developing red cells with nuclear maturation arrested due to impaired DNA synthesis.
- Commonest causes: Vitamin B12 deficiency and Folate deficiency.
- Involves the entire haemopoietic system, not just red cells.
- B12 deficiency can exist before overt anaemia develops (neurological features may precede).
🩺 Aetiology & Causes
| Macrocytosis with Megaloblasts (true megaloblastic) |
- Vitamin B12 deficiency (pernicious anaemia, malabsorption, gastrectomy, ileal disease)
- Folate deficiency (poor diet, alcoholism, malabsorption, increased demand e.g. pregnancy)
|
| Macrocytosis without Megaloblasts (non-megaloblastic) |
- Liver disease, Alcohol excess 🍷
- Aplastic anaemia, Sideroblastic anaemia
- Myeloid leukaemia, Myeloma
- Physiological: Pregnancy, Newborns
- Hypothyroidism 🧠
- Drugs: Methotrexate, Azathioprine, Hydroxyurea, Zidovudine, ddI/ddC
|
🔎 Investigations
- Blood counts: Low Hb, MCV >96 fl, often pancytopenia.
- Blood film: Hypersegmented neutrophils, oval macrocytes.
- LDH ↑ markedly (due to ineffective erythropoiesis).
- Reticulocyte count ↓ (underproduction).
- Serum B12 & Folate: to distinguish the cause.
- Bone marrow: Megaloblasts (if unclear diagnosis).
💊 Management
- Treat the underlying cause (e.g., dietary deficiency, malabsorption, pernicious anaemia).
- Always replace B12 before (or with) folate if both are low → prevents neurological complications.
- B12 replacement: Hydroxocobalamin IM injections (NICE: 1 mg IM alternate days × 2 weeks, then every 3 months for life in pernicious anaemia).
- Folate replacement: Folic acid 5 mg daily (after ruling out isolated B12 deficiency).
- Monitor Hb, reticulocyte response, and symptoms.
Cases - Macrocytic Anaemia
- Case 1 - Vitamin B12 Deficiency (Pernicious Anaemia):
A 65-year-old woman presents with tiredness, glossitis, and numbness in her feet. FBC: Hb 8.5 g/dL, MCV 112 fL. Peripheral smear: macro-ovalocytes and hypersegmented neutrophils. Serum B12 low, intrinsic factor antibodies positive. Diagnosis: Macrocytic anaemia due to pernicious anaemia.
- Case 2 - Folate Deficiency (Dietary):
A 25-year-old man with a history of alcohol misuse presents with pallor and mild jaundice. FBC: Hb 9.2 g/dL, MCV 118 fL. Serum folate low, B12 normal. Diagnosis: Macrocytic anaemia from folate deficiency, likely nutritional/alcohol related.
- Case 3 - Alcohol and Liver Disease:
A 50-year-old man with chronic liver cirrhosis presents with fatigue. FBC: Hb 10.0 g/dL, MCV 110 fL. Blood film: target cells and macrocytes. LFTs abnormal. Diagnosis: Macrocytic anaemia due to alcohol-related liver disease.
- Case 4 - Myelodysplastic Syndrome (MDS):
A 72-year-old man presents with anaemia and recurrent infections. FBC: Hb 8.9 g/dL, MCV 105 fL, neutropenia, thrombocytopenia. Blood film: dysplastic changes. Bone marrow: hypercellularity with dysplastic precursors. Diagnosis: Macrocytic anaemia as part of MDS.
- Case 5 - Drug-Induced (Methotrexate):
A 58-year-old woman with rheumatoid arthritis on methotrexate presents with fatigue. Hb 9.4 g/dL, MCV 108 fL. Folate levels reduced. Diagnosis: Macrocytic anaemia secondary to folate antagonism (methotrexate).
Teaching Commentary 📘
Macrocytosis is defined as MCV >100 fL. Causes can be divided into megaloblastic (B12 or folate deficiency impairing DNA synthesis) and non-megaloblastic (alcohol, liver disease, hypothyroidism, drugs, MDS). Blood film clues: hypersegmented neutrophils in megaloblastic anaemia; target cells in liver disease; dysplasia in MDS. Always check B12 before starting folate replacement, as unopposed folate can worsen neurological deficits. Management focuses on cause: lifelong B12 injections in pernicious anaemia, folate replacement in deficiency, alcohol cessation, or disease-specific therapy (e.g., MDS supportive/transplant).
