
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Cerebral Venous Thrombosis (CVT)
Related Subjects: Thrombophilia testing |Antiphospholipid syndrome |Protein C Deficiency |Protein S Deficiency |Prothrombin 20210A mutation |Factor V Leiden Deficiency |Antithrombin III deficiency (AT3) |Cerebral Venous Sinus thrombosis |Budd-Chiari syndrome |Acute Hydrocephalus
🧠 Cerebral Venous Thrombosis (CVT) is an under-recognised cause of stroke, especially in young adults, postpartum women, and patients with prothrombotic conditions. ⚠️ Postpartum period is a major risk factor, and CVST has also been reported rarely in association with COVID-19 vaccination + thrombocytopenia. Clues: persistent headache, papilloedema, seizures, or infarcts not in arterial territories.
📖 About
- Likely underdiagnosed; many cases are missed or treated late.
- Headache + papilloedema + normal CT should raise suspicion.
- Think of CVST in pregnant/postpartum women or patients with prothrombotic risk factors.
⚙️ Aetiology (Causes)
- 💊 OCP use, pregnancy, postpartum period.
- 💉 Procoagulant states: Factor V Leiden, protein C/S deficiency, antithrombin deficiency, prothrombin mutation, hyperhomocysteinaemia.
- 🩸 Haematological: polycythaemia, thrombocythaemia, leukaemia, sickle cell disease.
- 🦠 Infections: mastoiditis, otitis media, sinusitis, bacterial meningitis.
- 🧬 Systemic conditions: Behçet’s, SLE, ulcerative colitis, Crohn’s, APS, Graves’ disease.
- ⚡ Drugs: Ecstasy (MDMA), chemotherapy.
- 🦴 Trauma/neurosurgery near venous sinuses.
- 🦠 Malignancy: adenocarcinomas, haematological cancers.
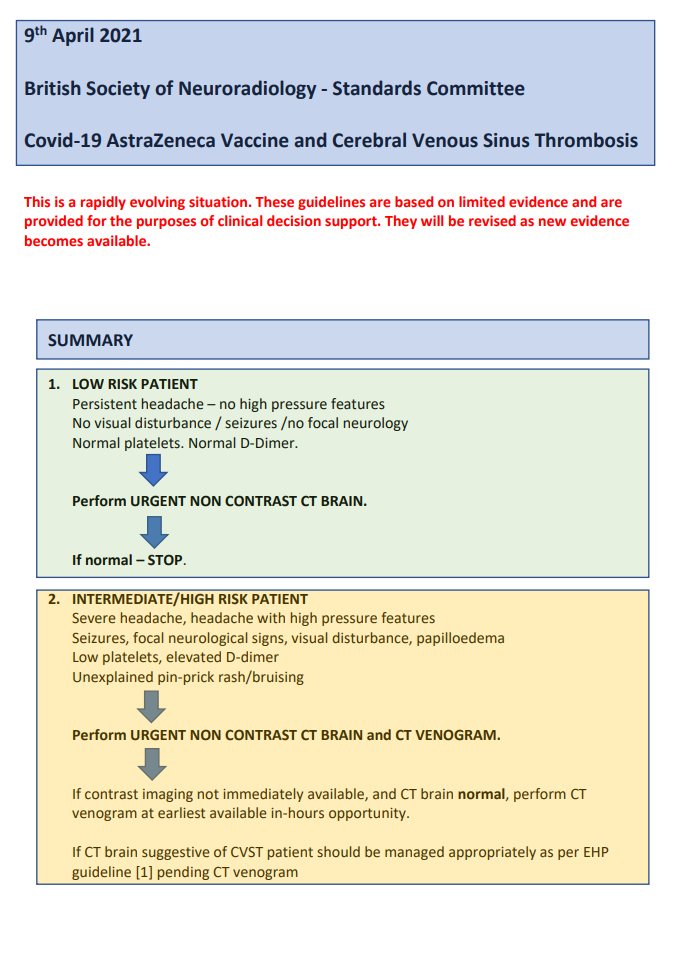
- 💉 Post-COVID-19 vaccine (rare): CVST with thrombocytopenia/VITT.
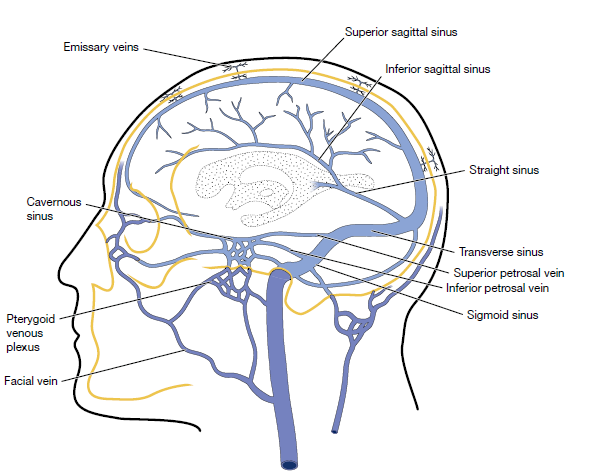
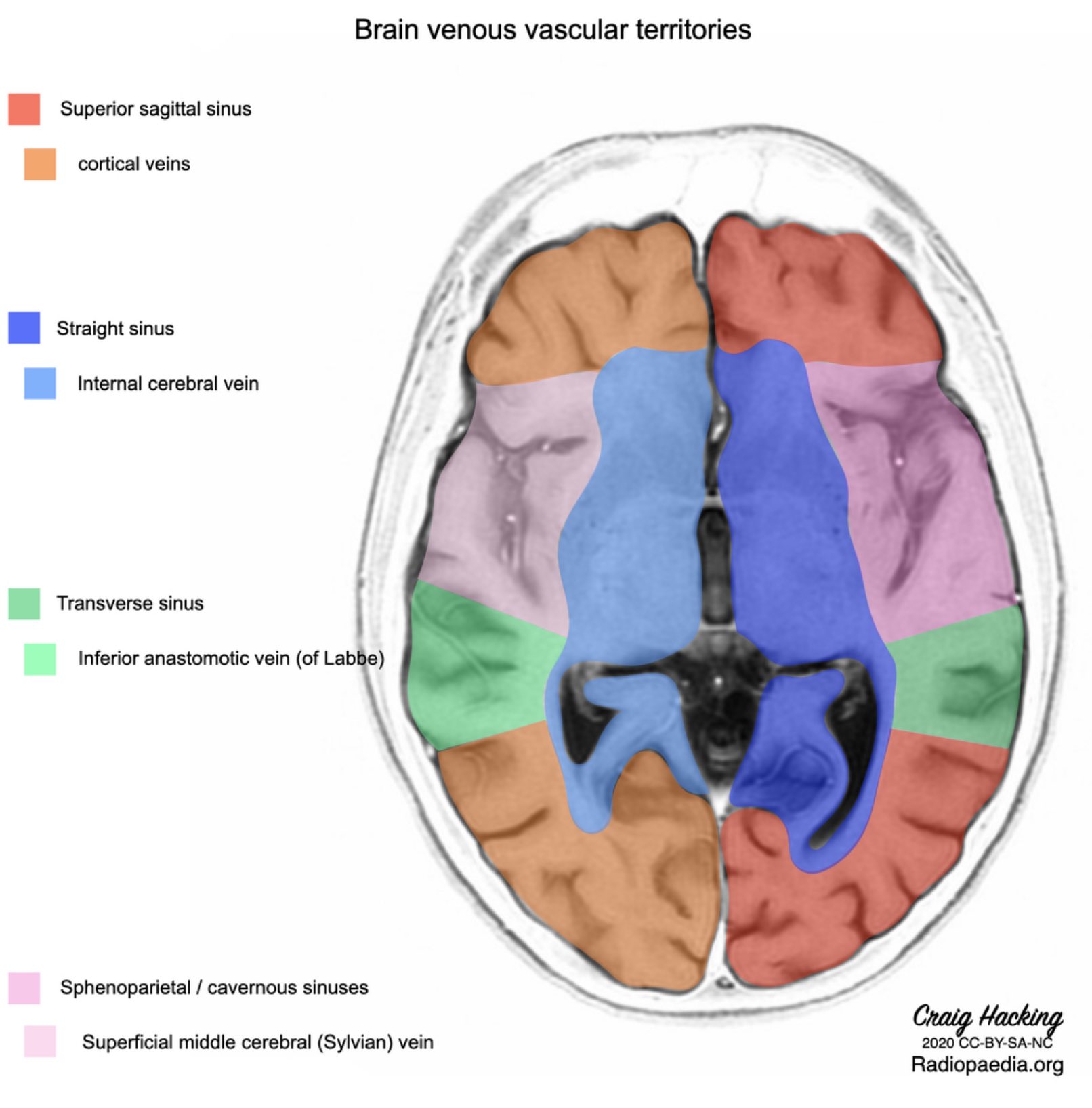
🧭 Venous Anatomy
CVST can affect any venous sinus or cortical vein, leading to raised ICP and venous infarction.
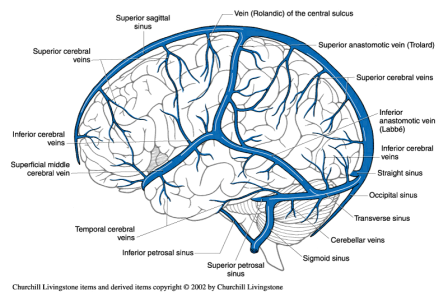
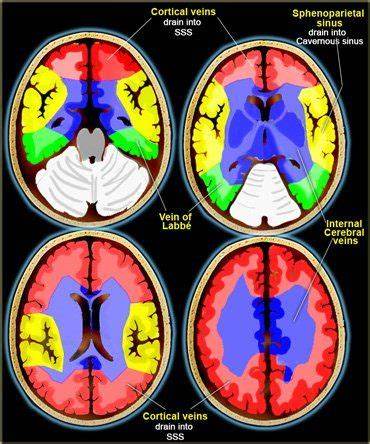
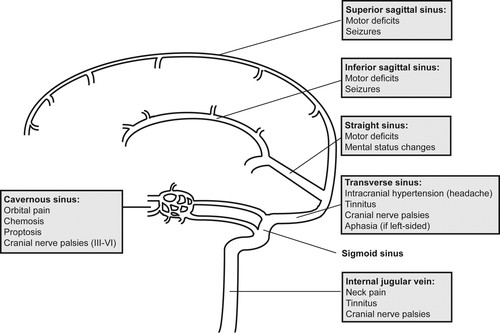
🩸 Common Sites & Clinical Patterns
- Superior sagittal sinus: raised ICP, headache, papilloedema.
- Lateral/straight sinus, vein of Galen: bilateral thalamic infarcts → akinetic mutism.
- Small cortical veins: focal cortical signs, seizures.
- Cavernous sinus: cranial neuropathies, proptosis, cavernous sinus syndrome.
🔬 Pathophysiology
- Obstruction of venous outflow → venous congestion, cytotoxic + vasogenic oedema.
- Haemorrhagic venous infarction due to capillary rupture.
- ↓ CSF absorption via arachnoid granulations → raised ICP.
- Subarachnoid haemorrhage may occasionally occur.
🩺 Clinical Presentation
- 💢 Headache in ~90% (often progressive, worse lying down).
- 🌡️ Raised ICP: papilloedema, nausea, vomiting, sixth nerve palsy.
- ⚡ Seizures: focal or generalised (much more common than in arterial stroke).
- 🧑⚕️ Focal neurology: hemiparesis, aphasia, cortical signs.
- 🤒 Cavernous sinus thrombosis: ophthalmoplegia, cranial nerve palsies, facial pain.
- 🌀 Atypical: psychosis, encephalopathy, TIA-like symptoms, migraine-like headache.
🧾 Differential Diagnosis
- Idiopathic intracranial hypertension (IIH): important mimic, especially in young obese women. ➡️ If male or non-obese, always exclude CVST.
🔍 Investigations
- 🩸 FBC: Look for thrombocytopenia (consider VITT, HIT, leukaemia).
- 🧪 D-dimer: Usually raised but not fully sensitive.
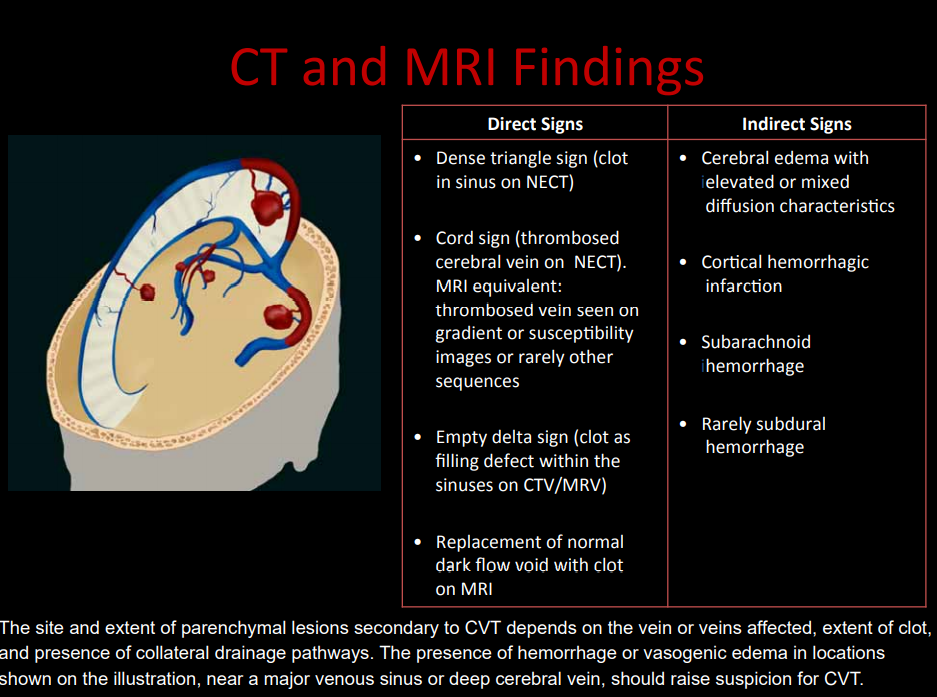
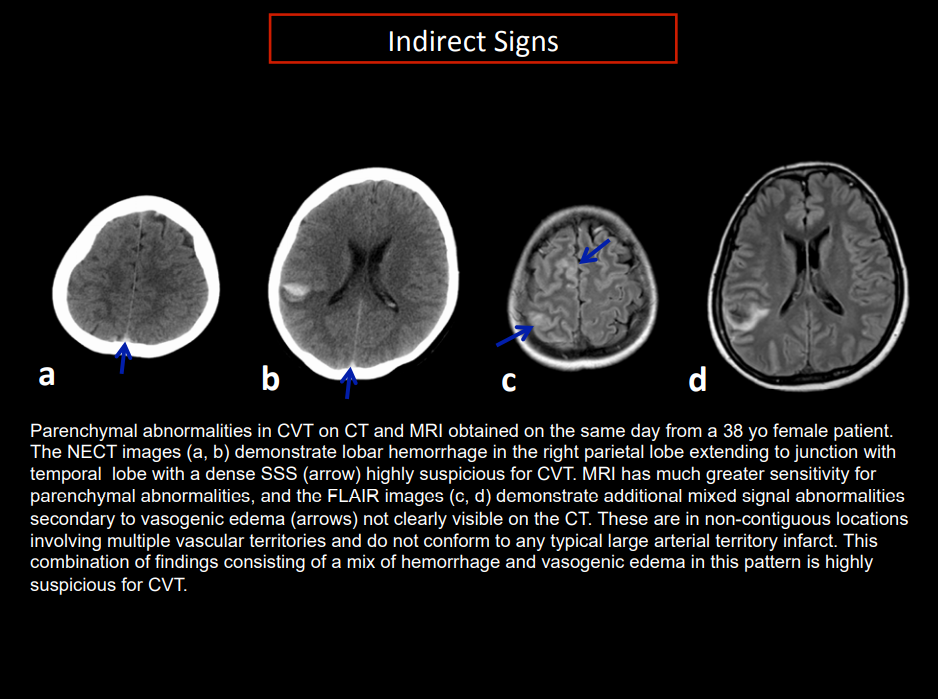
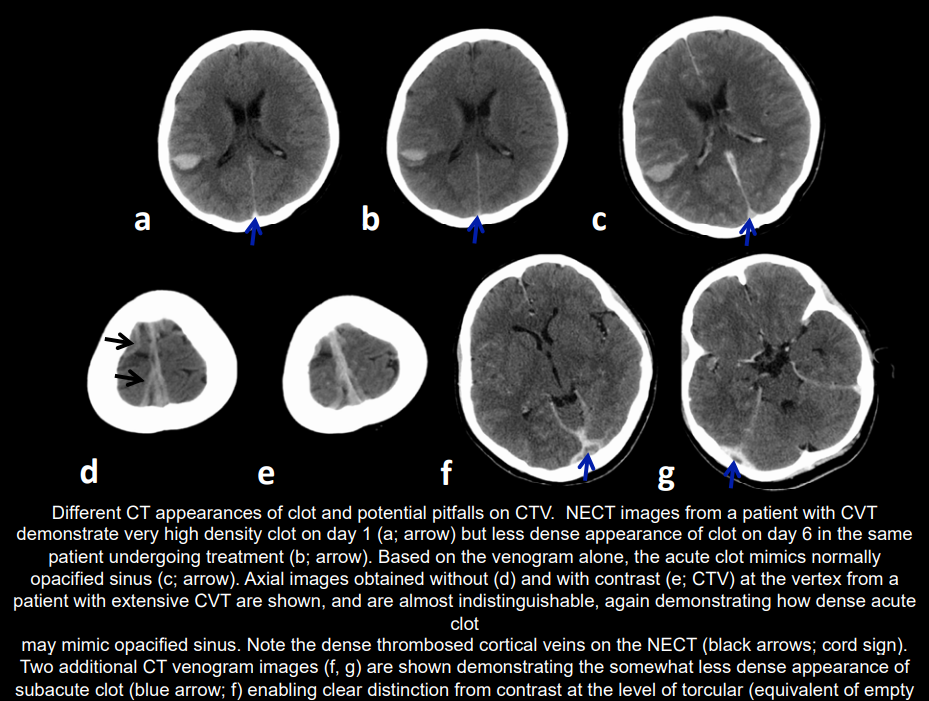
- 🖼️ CT (plain): May be normal; may show haemorrhagic infarcts not in arterial territories. "Cord sign" (fresh clot), SAH possible.
- 🩻 CT venography: "Empty delta sign" (contrast around clot in sagittal sinus).
- 🧲 MRI/MRV: Best modality. Detects venous clot, oedema, infarction, haemorrhage.
- 💉 CSF: ↑ opening pressure, ↑ protein; WCC mildly raised.
- 🧬 Thrombophilia screen: Factor V Leiden, prothrombin G20210, protein C/S deficiency, antithrombin deficiency, homocystinuria.
 alt="CT Venous Image 1"
style="display:block; width:100%; max-width:100%; height:auto; margin:10px auto; border-radius:8px;">
alt="CT Venous Image 1"
style="display:block; width:100%; max-width:100%; height:auto; margin:10px auto; border-radius:8px;">
📉 Prognosis Factors
- Deep venous involvement → poor prognosis (bilateral thalamic infarcts).
- Male sex associated with worse outcomes.
- Right lateral sinus thrombosis carries higher risk.
🧬 Inherited Procoagulant Conditions (approx. prevalence)
- Factor V Leiden: 3–7%.
- Prothrombin G20210 mutation: 1–2%.
- Protein C deficiency: 0.3%.
- Protein S deficiency: 0.1%.
- Antithrombin deficiency: 0.02%.
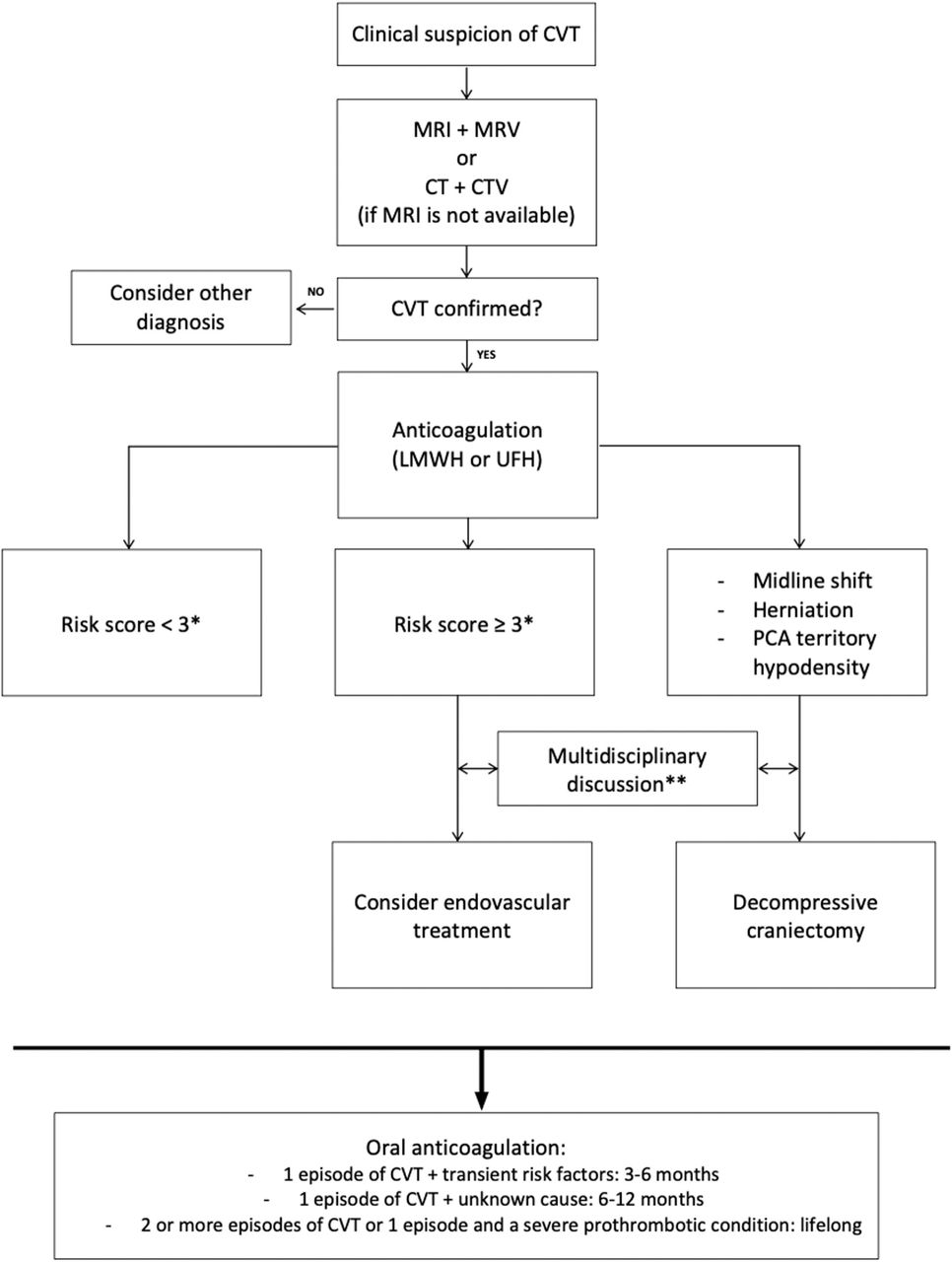
⚖️ Management
- 💉 Anticoagulation is the cornerstone: LMWH preferred (BID dosing). UFH if renal failure or rapid reversal required.
- 🩸 Even with haemorrhagic venous infarcts, anticoagulation is not contraindicated.
- 🔄 Oral anticoagulation (warfarin, INR 2–3) for 3–12 months; longer if recurrent or idiopathic.
- ⚡ Endovascular thrombolysis/thrombectomy: for severe/refractory cases in expert centres.
- 📉 COVID-19 related (VITT): avoid heparin, use IVIG + non-heparin anticoagulants (e.g., argatroban, fondaparinux) per guidelines.
- 🧑⚕️ Supportive: ICP management (acetazolamide, CSF drainage if needed), seizure prophylaxis if recurrent.
📚 References
- Cerebral venous thrombosis: a practical guide. Pract Neurol 2020.
- Imaging Approach to CVST – CAR.
- Piazza G. Circulation 2012;125:1704–1709.
- ACC: CVST with Vaccine-Induced Thrombocytopenia.
💡 Exam Pearls:
– CVST = young woman + headache + seizures + haemorrhagic infarct not in arterial territory.
– Always request CT/MR venography if suspicion is high.
– Anticoagulation is safe, even with haemorrhage.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery