
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
ECG - ST-T T waves changes
Related Subjects: |ECG Basics |ECG Axis |ECG Analysis |ECG LAD |ECG RAD |ECG Low voltage |ECG Pathological Q waves |ECG ST/T wave changes |ECG LBBB |ECG RBBB |ECG short PR |ECG Heart Block |ECG Asystole and P wave asystole |ECG QRS complex |ECG ST segment |ECG: QT interval |ECG: LVH |ECG RVH |ECG: Bundle branch blocks |ECG Dominant R wave in V1 |ECG Acute Coronary Syndrome |ECG Crib sheets
📖 T Waves
- ⚡ The T wave represents ventricular repolarisation.
- 🧭 Normally, T waves are concordant with the QRS (same direction), except in aVR and V1 where inversion can be normal.
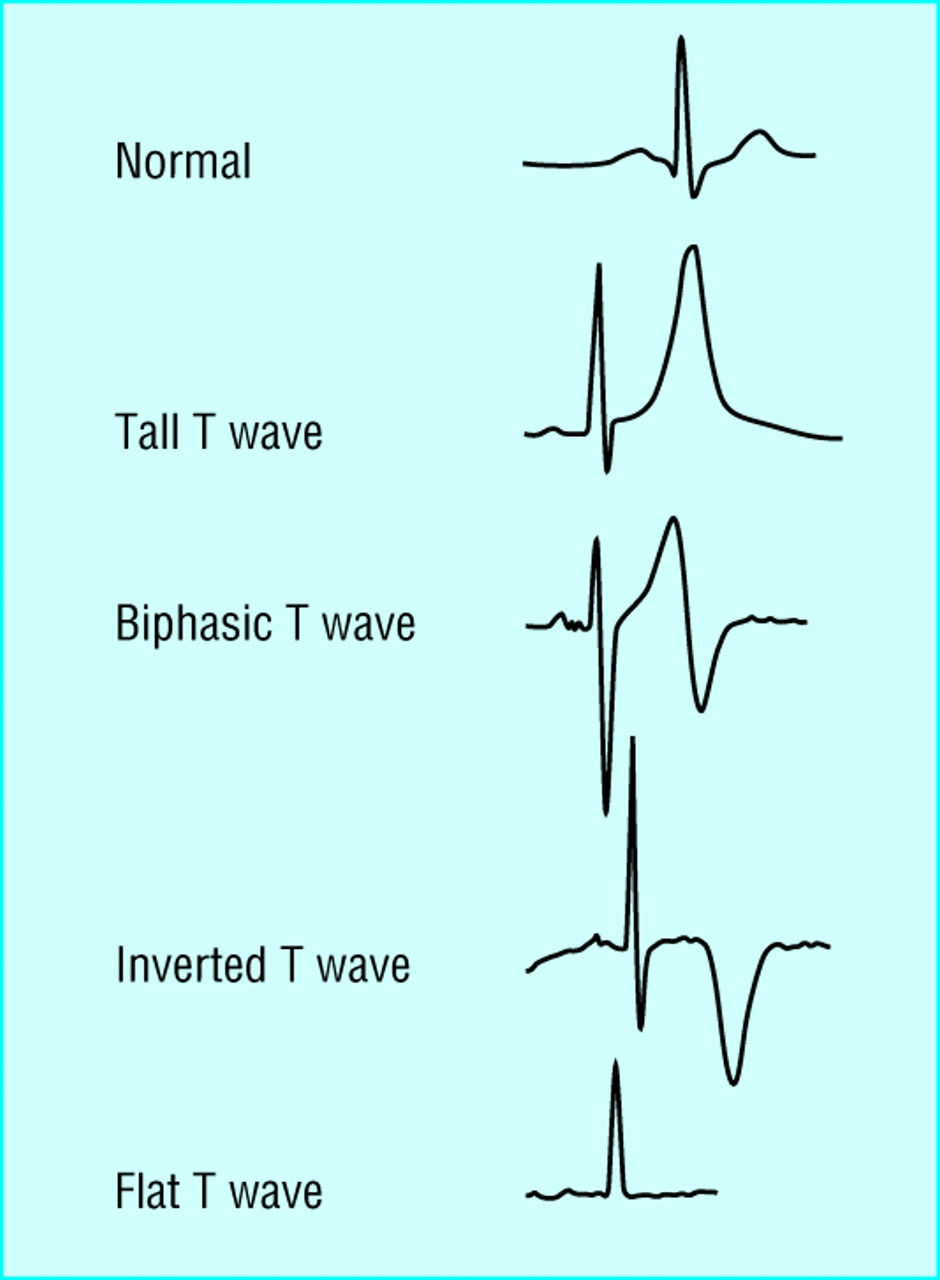
⚠️ Abnormal T Wave Patterns
- 📈 Peaked T waves: Classic for hyperkalaemia (tall, narrow, “tent-shaped”).
- ⬇️ Flattened T waves: Seen in hypokalaemia, hypothyroidism, obesity, COPD.
- ⬇️⬇️ Deep T wave inversion:
- Acute Coronary Syndrome (ischaemia)
- Left Ventricular Hypertrophy (strain pattern)
- Left Bundle Branch Block
- Hypertrophic Cardiomyopathy
- 🔺 Deep anterior T wave inversion: LAD stenosis, Subarachnoid haemorrhage (neurogenic T waves), Takotsubo cardiomyopathy.
- 🔻 Deep inferior T wave inversion: Suggests RCA stenosis.
🛠️ Action
- 🧪 Always check electrolytes (K⁺, Mg²⁺, Ca²⁺) and correct if abnormal.
- 📉 Consider ischaemia if inversion is new, deep, or localized to vascular territories.
- 🧠 Think of extra-cardiac causes (e.g. SAH, stress-induced cardiomyopathy) if distribution is atypical.
💡 Teaching Pearls
✔️ Hyperkalaemia ➝ tall tented T waves are often the first ECG change (progress to sine-wave if severe). ✔️ Hypokalaemia ➝ flat T + U waves. ✔️ Deep T inversion in anterior leads can be ischaemic or neurogenic - always interpret in context!
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery