Related Subjects:
|Chest drain Insertion (Thoracostomy)
|Simple Needle Aspiration for Spontaneous Pneumothorax
|Pleural tap (thoracentesis)
🚨 Immediate Actions - Tension Pneumothorax
| Step |
Action |
Key Points |
Exam Pearls |
| 1️⃣ Recognise |
Clinical diagnosis |
Sudden dyspnoea, absent breath sounds, hyper-resonance, raised JVP,
hypotension, tracheal deviation (late sign)
|
Do NOT wait for chest X-ray |
| 2️⃣ Call for Help |
Activate emergency response |
Senior support + resus team |
Time-critical emergency |
| 3️⃣ ABCDE |
Start immediate resuscitation |
Airway assessment, 15L O₂ via non-rebreather mask,
monitoring (SpO₂, BP, ECG)
|
Treat simultaneously while diagnosing |
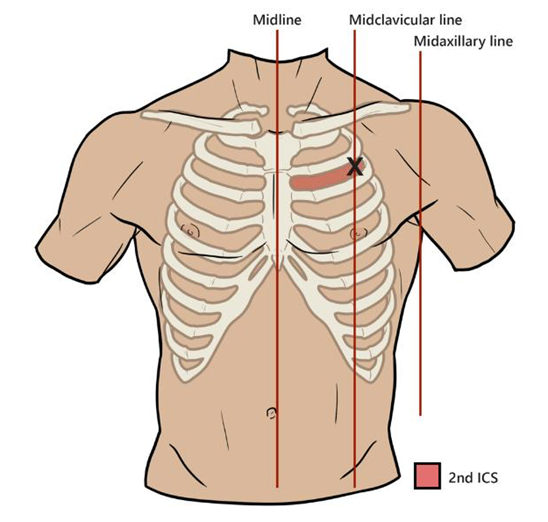
| 4️⃣ Needle Decompression |
Immediate decompression |
2nd ICS mid-clavicular line OR
4th/5th ICS anterior axillary line
|
Listen for “hiss” of escaping air |
| 5️⃣ Chest Drain |
Definitive management |
Insert in safe triangle |
Do not delay for imaging |
| 6️⃣ Reassess |
Monitor response |
Check vitals, breath sounds, oxygenation,
ensure drain functioning
|
Consider alternative diagnosis if no improvement |
🫁 Overview
- Life-threatening form of pneumothorax.
- Requires urgent needle decompression.
- “Hiss” of escaping air supports diagnosis.
- If no tension present → minimal harm; remove needle and reassess.
⚙️ Pathophysiology
- Air enters pleural space but cannot escape (one-way valve mechanism).
- Progressive pressure rise compresses lung and mediastinum.
- If intrathoracic pressure exceeds venous filling pressure → obstructive shock.
🧾 Causes
- 💥 Trauma: Penetrating (stab wounds, rib fractures) or Blunt trauma (e.g. RTA)
- ⚕️ Iatrogenic
- Central line insertion
- Lung biopsy / bronchoscopy
- Percutaneous tracheostomy
- Positive pressure ventilation (barotrauma)
- CPR, intercostal nerve block, thoracocentesis
- 🌊 Environmental Diving or Flying
- 🌀 Atraumatic
- Primary (young, tall, thin)
- Secondary (COPD, fibrosis, malignancy)
👩⚕️ Clinical Features
- Sudden dyspnoea and pleuritic chest pain.
- Tachycardia ❤️🔥. Respiratory distress, anxiety.
- Reduced/absent breath sounds on affected side.
- Hyper-resonant percussion note.
- Tracheal deviation away from affected side (late).
- Raised JVP. Hypotension → pre-arrest sign.
- Subcutaneous emphysema may be present.
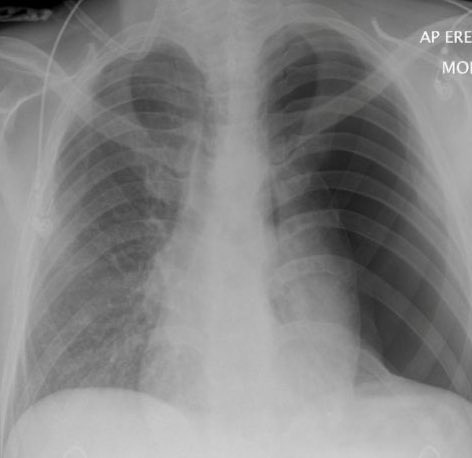
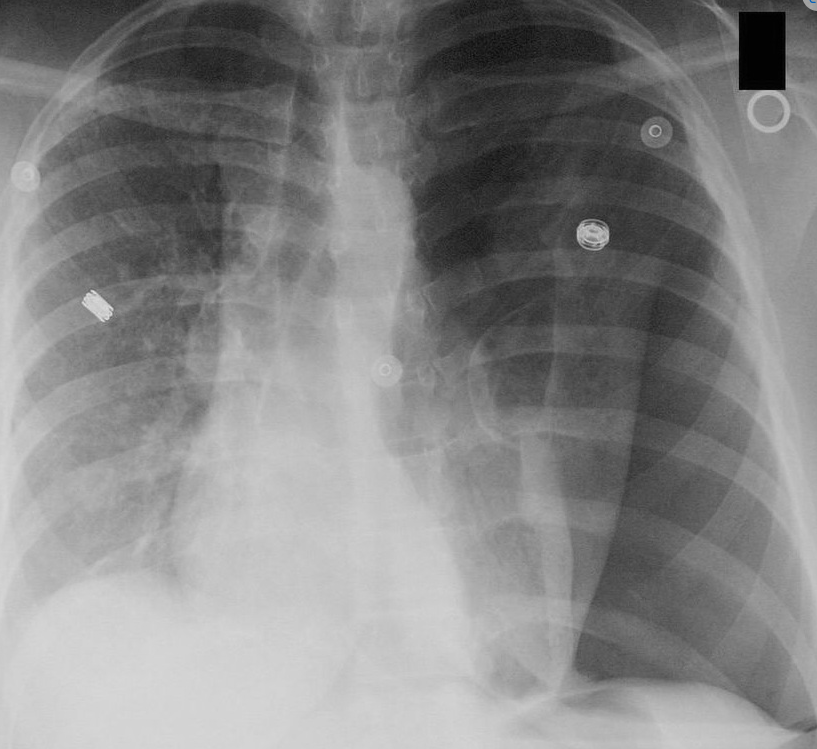
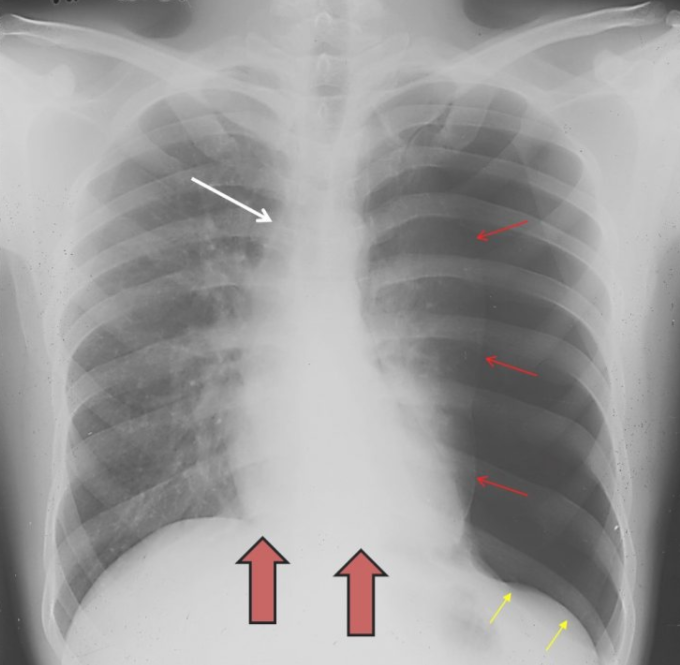
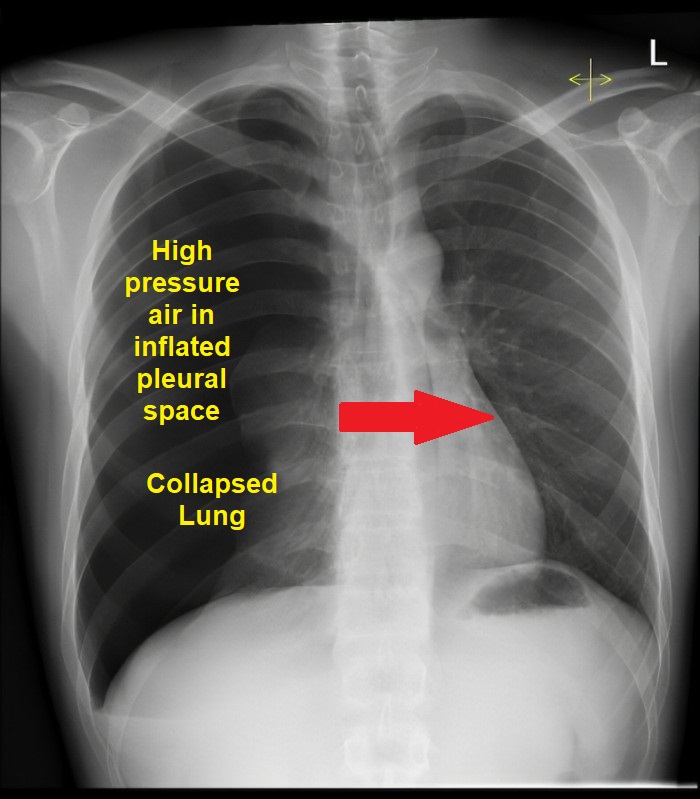
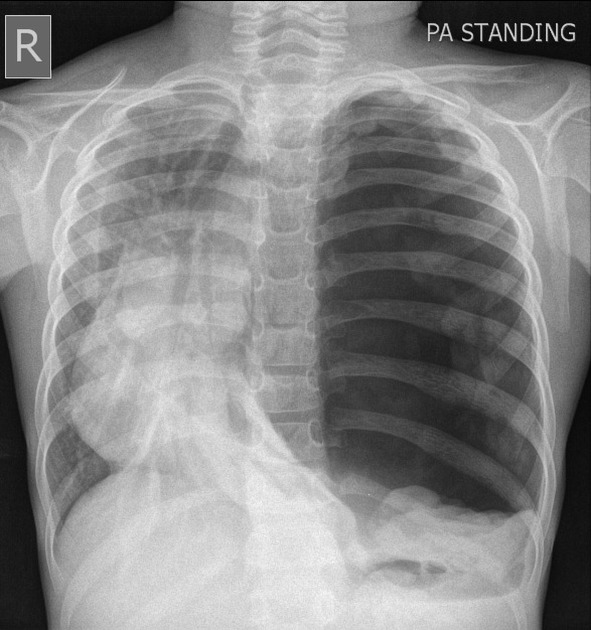
📸 Imaging (If Stable)
Do NOT delay treatment for imaging.
- Visible visceral pleural line.
- Absent lung markings peripherally.
- Collapsed ipsilateral lung.
- Mediastinal shift away.
- Flattened hemidiaphragm.
- Subcutaneous emphysema.
Ultrasound: ~94% sensitive, 100% specific
Absent lung sliding + “lung point” sign.
🛠️ Management
⚡ Immediate ABCDE
- Sit upright and start 15 L/min O₂ via non-rebreather mask.
- 💉 Emergency Needle Decompression Do not wait for imaging if the patient is unstable. Modern trauma teaching often uses 4th or 5th ICS, just anterior to the mid-axillary line. This is around the level of the nipple in males / inframammary fold area, but always count ribs if possible. Alternative is 2nd ICS mid-clavicular line, but failure rates can be higher because the chest wall is thicker and landmarking is often poor. Current sources describe both sites, with 4th/5th ICS anterior-to-mid-axillary or mid-axillary region increasingly preferred in trauma algorithms. Use a long large-bore cannula, often 14G/10–14G depending on local kit. Insert perpendicular to chest wall, just above the rib. Advance until air escapes / “hiss” is heard. Advance catheter over needle into pleural space. Remove needle, leave cannula in place.
🩺 Definitive Treatment
- Chest drain in safe triangle. Do not wait for CXR.
- Monitor for recurrence or drain blockage.
Landmarks
🧠 Cases - Tension Pneumothorax
- Case 1 - Trauma 🚑: High-speed RTA. Agitated, RR 36, absent left breath sounds, trachea deviated right, JVP raised, SpO₂ 78%. Immediate needle decompression → chest drain.
- Case 2 - Iatrogenic 💉: COPD patient collapses during CVC insertion. Hypotension, distended neck veins, absent breath sounds. Rapid decompression is life-saving.
- Case 3 - Cardiac Arrest 🫀: Ventilated ITU patient develops PEA. High airway pressures, unilateral absent breath sounds. Immediate bilateral decompression during ALS.
🩺 Exam Tip:
Tension pneumothorax = obstructive shock.
Treat first. Confirm later.
Needle decompression saves life. Chest drain is definitive.
