Related Subjects:
|Ectopic Pregnancy
⚠️ Ectopic pregnancy must be suspected in any woman of reproductive age with a positive pregnancy test, amenorrhoea, lower abdominal/pelvic pain, or abnormal vaginal bleeding. Delayed diagnosis can be life-threatening.
📖 Overview
- 🚺 Leading cause of maternal death in the first trimester.
- 💡 Classic triad: positive β-HCG, amenorrhoea, empty uterus on ultrasound.
- 🧪 Normal early pregnancy: serum β-HCG doubles approximately every 48 hours. Plateauing or slow rise is suspicious for ectopic.
- ⚠️ Avoid routine digital vaginal examination until resuscitation is available, as manipulation can precipitate rupture.
🧬 Aetiology & Sites
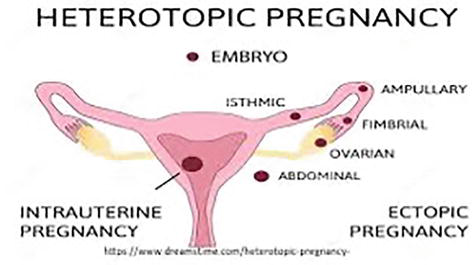
- Implantation of the embryo outside the uterine cavity.
- 📍 ~90% occur in the fallopian tube (most commonly ampullary region); others: cervical, interstitial, ovarian, abdominal.
- Incidence: ~1 in 200 pregnancies; risk increases with maternal age.
⚡ Risk Factors
- Previous ectopic pregnancy
- Pelvic inflammatory disease (PID), endometriosis, prior tubal surgery
- Use of IUCD
- Fertility treatments: IVF, reversal of sterilisation
- Ovarian/uterine cysts or tumours
- Smoking 🚬
🩺 Clinical Features
- Pre-rupture: Amenorrhoea (5–8 weeks post-LMP), unilateral sharp lower abdominal pain, light PV bleeding (“prune-juice” colour), nausea, breast tenderness.
- Post-rupture: Hypotension, tachycardia, syncope, shoulder-tip pain (diaphragmatic irritation), peritonitis → emergency.
- Vasovagal episodes and collapse may be initial presentation in some cases.
🔬 Investigations
- 🧪 Serum β-HCG: Serial measurement; plateau or suboptimal rise suggests ectopic.
- 🔎 Transvaginal ultrasound: Empty uterus, adnexal mass, free fluid in pelvis or pouch of Douglas.
- 💉 Rhesus typing: Anti-D prophylaxis indicated for Rh-negative women.
- 🩺 Laparoscopy: definitive diagnosis if imaging and β-HCG are inconclusive.
- Additional: CBC, blood group, renal and liver function if planning methotrexate.
🔍 Differential Diagnosis
- Acute appendicitis
- Acute PID or tubo-ovarian abscess
- Threatened, incomplete, or missed miscarriage
- Ovarian torsion
💊 Management
- Medical (stable, unruptured):
- Methotrexate single-dose protocol: for β-HCG <1500 IU/L, mass <4 cm, no fetal cardiac activity, and hemodynamically stable.
- Monitor β-HCG at day 4 and day 7; expect ≥15% fall between measurements. Repeat weekly until negative.
- Side effects: nausea, stomatitis, fatigue; counsel on avoiding alcohol and folic acid supplementation.
- Surgical:
- Laparoscopy: salpingotomy (preserve tube) or salpingectomy (remove tube) for stable patients.
- Emergency laparotomy + salpingectomy if unstable, ruptured, or peritonitic.
- Conservative / expectant:
- Small (<2 cm), asymptomatic masses, β-HCG <1000 IU/L.
- Serial β-HCG and ultrasound; decline ≥15% per week expected.
- Supportive:
- IV fluids and blood transfusion if hypotensive or shocked.
- Anti-D prophylaxis for Rh-negative women (250 IU IM) if indicated.
- Referral to Early Pregnancy Assessment Unit (EPAU) for follow-up until β-HCG negative.
📚 NICE & RCOG References