
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Death Certificates and Cremation UK
💐 Please be kind to the bereavement office staff. They’re doing a difficult job under pressure. Any delays almost always land on grieving families - not on “the system”. If you’re unsure about the cause of death, pause and speak to your registrar or consultant. (See also: Confirming Death.)
📜 Death Certification in England (2026 - What’s Changed)
- All deaths now go through the Medical Examiner (ME) system.
- The ME provides independent scrutiny of the cause of death and speaks to the bereaved.
- This is designed to improve accuracy, safety, and transparency - not to catch you out.
👩⚕️ Who Can Complete a Medical Certificate of Cause of Death (MCCD)
- A doctor who attended the patient during their last illness and has seen them within 28 days before death (⚠️ updated from the old 14-day rule).
- You must be reasonably confident of the cause of death.
- If uncertain - always discuss with your senior before completing the MCCD.
- The MCCD is then reviewed by the Medical Examiner before registration.
⚖️ When to Involve the Coroner
- When in doubt, discuss with the coroner’s officer. They will guide you.
- Sometimes they will advise you to proceed with the certificate.
- Other times, they may direct a coroner’s post-mortem or inquest.
🚩 Common Indications for Coroner Referral
- Cause of death unknown or unclear.
- Patient not seen by a doctor within the last 28 days.
- Death within 24 hours of admission.
- Deaths related to surgery, anaesthesia, procedures, or treatment complications.
- Suspicious circumstances: assault, neglect, alleged negligence.
- Trauma: falls, accidents, industrial injury.
- Road traffic collisions.
- Deaths due to violence, suicide, poisoning (including alcohol).
- Deaths in custody or during arrest.
- Deaths due to industrial or occupational disease.
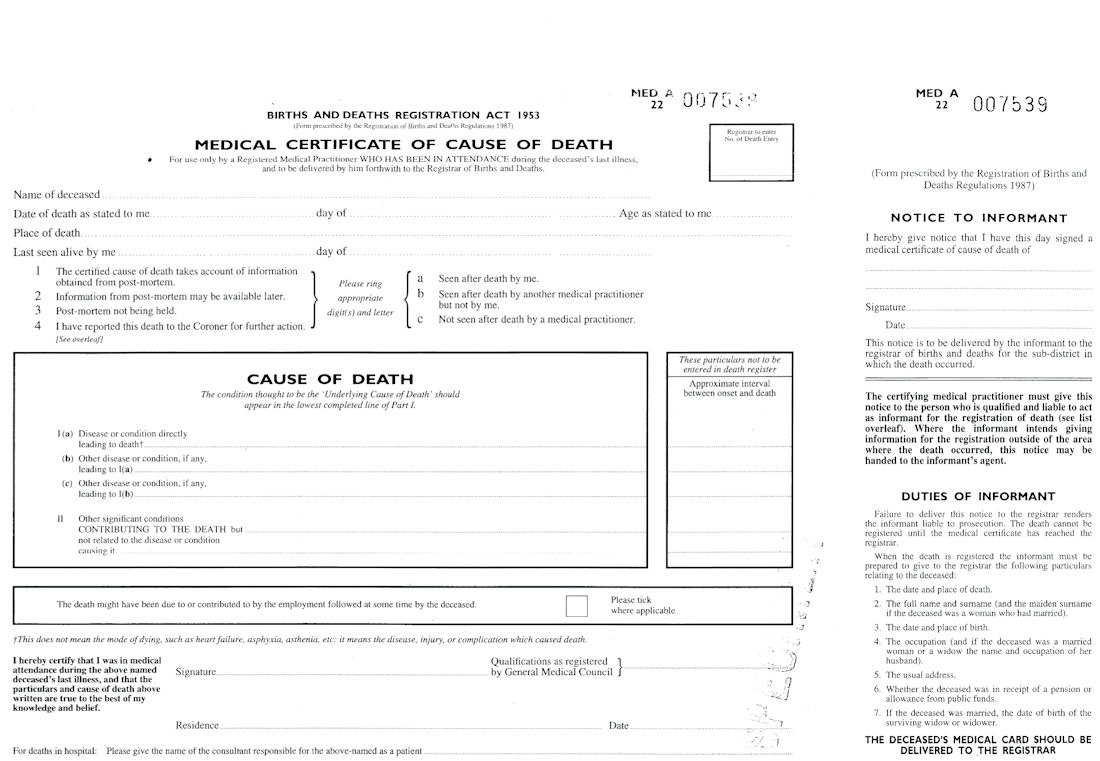
🖊️ Completing the Cause of Death (This Matters)
- Part I(a): The direct cause of death
✔ e.g. Pulmonary embolism, Myocardial infarction, Bronchopneumonia
✖ Not acceptable: cardiac arrest, respiratory failure, syncope, shock - Part I(b): The condition leading to I(a)
✔ e.g. Fractured neck of femur, Ischaemic heart disease
Leave blank if I(a) is sufficient - Part I(c): The underlying cause of I(b)
✔ e.g. Osteoporosis - Part II: Other significant contributing conditions
✔ Diabetes, Morbid obesity, COPD, IHD
⚠️ Practical Pitfalls (Learned the Hard Way)
- 🚫 No abbreviations: write “pulmonary embolism”, not PE; “myocardial infarction”, not MI; “fractured neck of femur”, not NOF.
- ✍️ Sign clearly and add your GMC number (good practice).
- 📋 Ask bereavement staff to check for simple errors - they’re very good at spotting them.
- 🦠 Always qualify disease properly: “Hepatitis” once led to unnecessary infectious precautions when it was actually alcoholic liver disease.
🧍 Identifying and Examining the Body
- You must personally identify the body.
- This usually involves uncovering the upper torso and checking the hospital ID band.
- Make sure you genuinely recognise the deceased - don’t just rely on notes.
🔥 Cremation-Specific Points
- Cremation permanently destroys physical evidence - so there are extra safeguards.
- You must see the body and review the notes carefully.
- ⚠️ Always check for pacemakers - usually below either clavicle. (They can explode during cremation.)
- Radioactive implants must also be identified and removed.
- Cremation forms require discussion with a second, independent doctor.
😔 Why accuracy matters: Incomplete or incorrect forms delay funerals, distress families, and create major problems for mortuary staff. Doing it carefully once saves everyone a lot of pain later.
📝 Practical On-Call Tip
- If burial vs cremation isn’t yet known, it’s often sensible to complete the cremation paperwork anyway.
- It avoids a second visit and prevents delays if cremation is later chosen.
🧠 Makindo bottom line: Death certification isn’t “just paperwork”. It’s a final clinical act for the patient - and a deeply important one for their family. Slow down, be accurate, escalate when unsure, and be kind to everyone involved.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery