Related Subjects:
|Wolff-Parkinson White syndrome (WPW) AVRT
|Lown Ganong Levine Syndrome AVRT
|Supraventricular Tachycardia (SVT)
|Atrioventricular Nodal Reentrant Tachycardia AVNRT
|Atrial Flutter
|Atrial Fibrillation
|Sinus Tachycardia
|Sinus Arrhythmia
|Multifocal Atrial Tachycardia
|Resuscitation - Adult Tachycardia Algorithm
|Resuscitation - Advanced Life Support
⚡ Supraventricular Tachycardia (SVT) is a group of rapid heart rhythms originating above the ventricles (atria or AV node).
🫀 While usually benign, it can cause distressing symptoms (palpitations, dizziness, syncope) and occasionally serious complications.
🎯 Correct diagnosis and management are essential to relieve symptoms and prevent adverse outcomes.
📌 About
- SVT = any tachycardia arising from above the Bundle of His.
- Mainly includes reentrant tachycardias such as AVRT and AVNRT.
- 🚶 Generally benign, but can mimic panic attacks and be disabling.
- 💉 Often curable with catheter ablation, especially in Wolff-Parkinson-White (WPW).
🔄 Aetiology of Reentrant SVT
- Needs two pathways (fast vs slow) ➝ reentrant circuit 🔄 like a Catherine wheel firework 🎆.
- Pathway properties:
- 🐢 Slow Pathway: Long refractory period.
- 🐇 Fast Pathway: Short refractory period.
- Classifications:
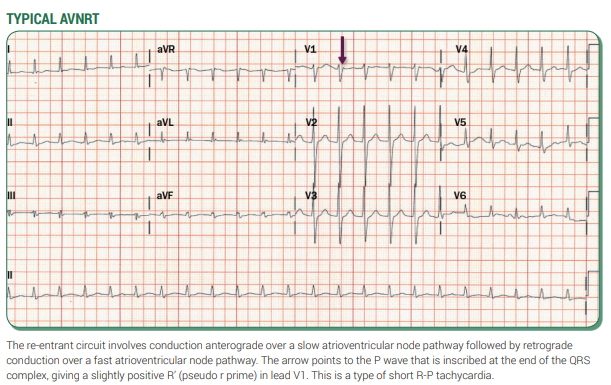
- ✅ Slow-Fast AVNRT: Most common (>90%).
- ⚡ Fast-Slow AVRT: 10–15%.
- 🔸 Slow-Slow AVRT: Rare (<5%).
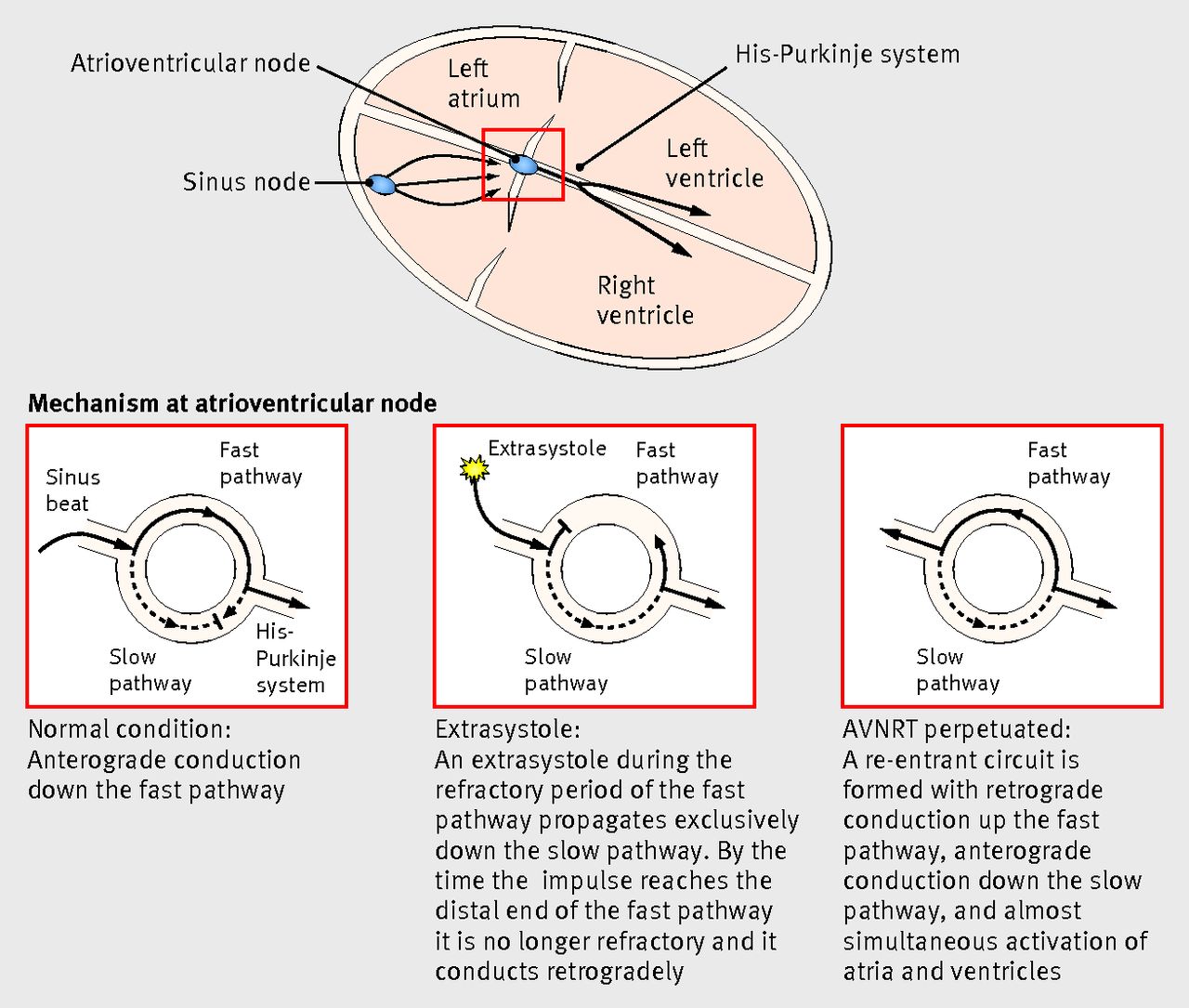
📊 Diagram – Pathways of AVRT and AVNRT
📖 Definition Includes
- ❤️ Sinus Tachycardia – from sinus node.
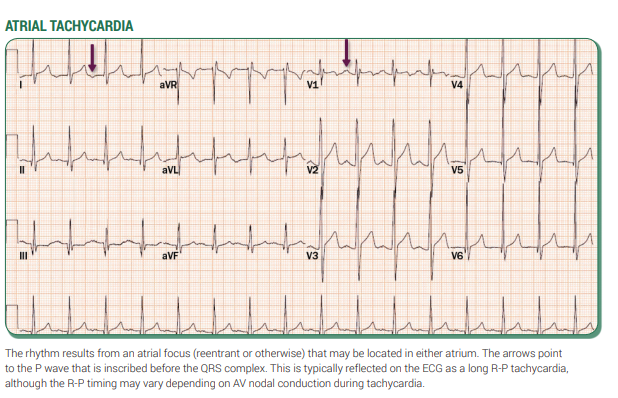
- ⚡ Atrial Tachycardia – ectopic atrial focus.
- 🎯 Multifocal Atrial Tachycardia – multiple atrial foci.
- ♻️ Atrial Fibrillation – chaotic atrial activity.
- 🔄 Atrial Flutter – reentry circuit, regular.
- But in practice, “SVT” usually means:
- AVNRT
- AVRT (often with WPW)
🧑⚕️ Clinical Features
- Seen in all ages; more common in women (M:F ~1:2).
- Symptoms:
- 💓 Palpitations
- 😵 Dizziness/lightheadedness
- 🫁 Dyspnoea
- 💢 Chest pain
- 💫 Syncope/presyncope
- Common triggers: ☕ caffeine, 🍷 alcohol, 🚬 smoking, stress, 💊 drugs.
🔍 Investigations
- 📊 ECG: Key test. Narrow complex tachycardia (120–240 bpm), may mimic VT if bundle branch block.
- 📈 Holter / Event Recorder: For transient episodes.
- 🧪 Labs: FBC, U&E, TFTs, LFTs.
- 🫀 Echocardiogram: Rule out structural disease.
- 🩻 CXR: Exclude lung causes if relevant.
- Consider 💡 pheochromocytoma if hypertension + SVT (rare).
💡 Clinical Pearls
- ⏱️ Sudden onset + sudden termination → classic PSVT.
- 👕 “Shirt-flapping” or “neck pounding” → highly suggestive of AVNRT.
- ⚠️ Hypotension/syncope → unstable → urgent treatment/referral.
- 🩺 WPW with delta waves → high risk ➝ ablation referral.
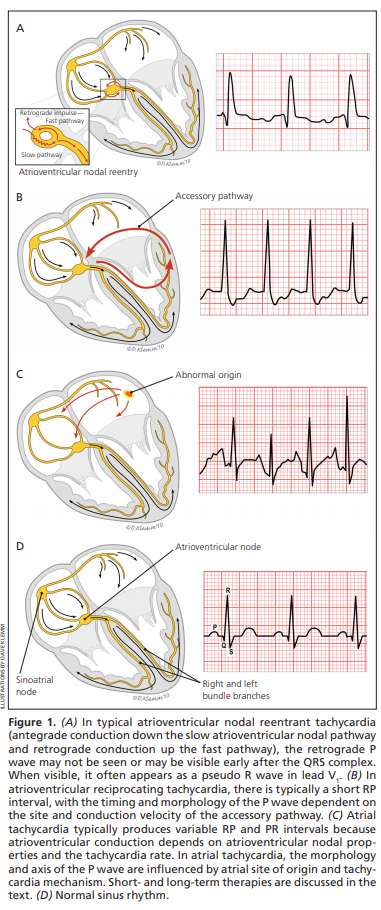
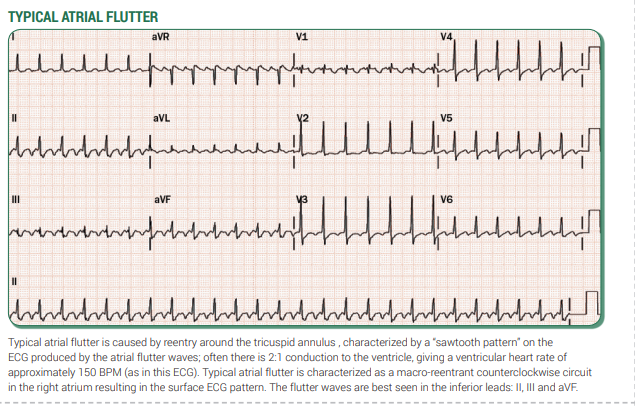
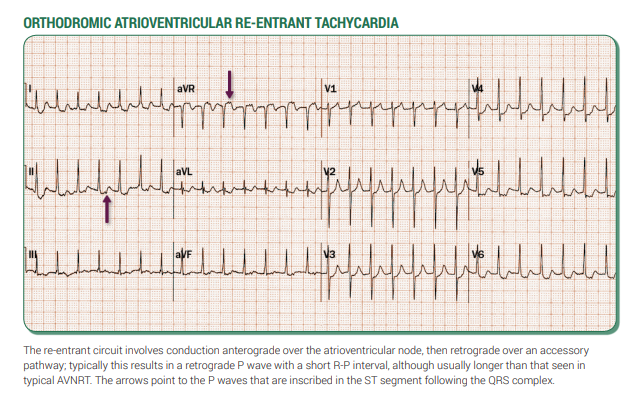
📊 Examples
🛠️ Management
- 🚑 Initial Assessment: ABC, IV access, urgent DC cardioversion if unstable.
- 🙂 Stable SVT:
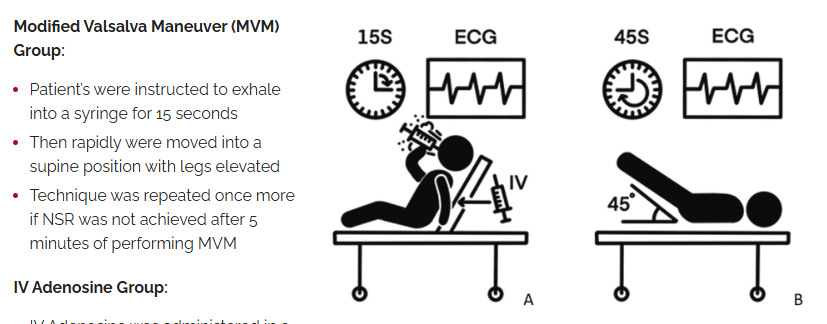
- 🙌 Vagal manoeuvres (Valsalva, carotid sinus massage, cold water face immersion).
- 💉 If fails → IV Adenosine (6 mg, then 12 mg if needed; warn about flushing & chest tightness).
 💊 Drugs:
💊 Drugs:
- 📉 Calcium channel blockers (IV verapamil, diltiazem).
- 🛡️ Beta-blockers in some cases (avoid in WPW + AF).
- ⚡ Amiodarone for broad/unstable SVT.
❌ Special Situations:
- WPW + AF ➝ avoid AV nodal blockers (adenosine, beta-blocker, digoxin, verapamil) ➝ use flecainide/propafenone/amiodarone or cardiovert.
🏥 Long-term:
- Electrophysiology referral for ablation in recurrent cases.
- Nodal ablation as last resort.
📚 References
