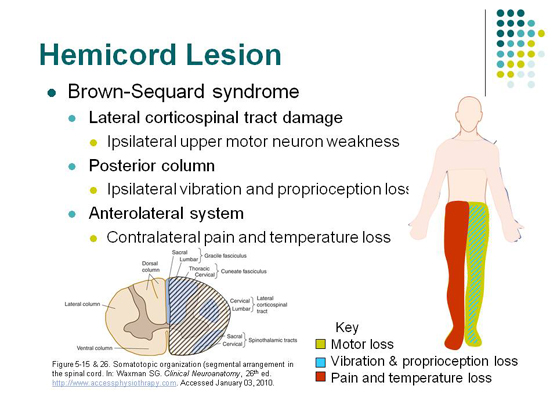
Brown-Sequard Spinal Cord syndrome
⚡ Rare neurological syndrome caused by a lesion affecting one half of the spinal cord (hemi-cord). 🧠 Produces a characteristic pattern: motor + dorsal column loss ipsilateral, spinothalamic loss contralateral.
ℹ️ About
- 🦠 Infection: e.g. Tuberculosis, syphilis
- 🔥 Inflammatory: Multiple sclerosis plaques, transverse myelitis
- 🎗️ Spinal tumours
- 🤕 Trauma: stab wounds, gunshot injuries, fracture-dislocation
- 💿 Disc herniation (rare unilateral cord compression)
🧬 Anatomy
- 🎯 Most often seen in the thoracic spine
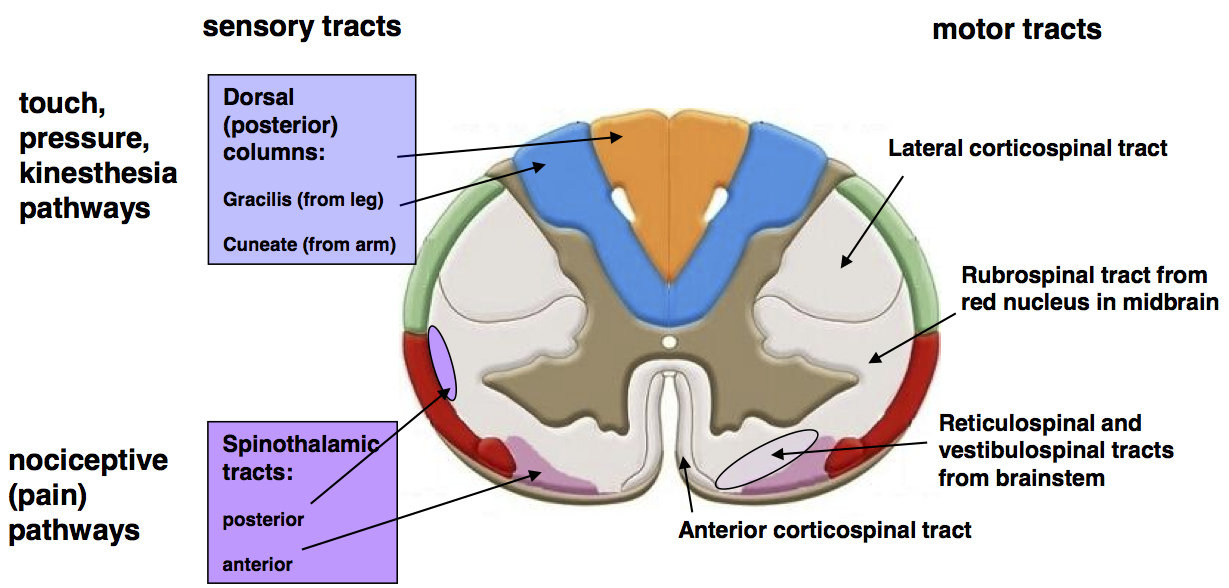
- 📌 Pathophysiology reflects interruption of:
– Corticospinal tract (motor, ipsilateral weakness)
– Dorsal columns (ipsilateral vibration, proprioception)
– Spinothalamic tract (contralateral pain & temperature)
🧪 Aetiology
- 📍 Unilateral spinal cord lesion (hemi-section or compression)
- 📊 Commonest level = thoracic region
🩺 Clinical Features
- 💪 Ipsilateral weakness/paralysis (UMN pattern: spasticity, hyperreflexia)
- 🦶 Ipsilateral loss of vibration, fine touch, proprioception
- 🔥 Contralateral loss of pain & temperature (spinothalamic fibres cross 1–2 levels above entry)
- 😮 Lesion above T1 → ipsilateral Horner’s syndrome (ptosis, miosis, anhidrosis)
- 🩹 Trauma cases often have associated injuries (fractures, vascular injury)
🔎 Investigations
- 🧪 Bloods: FBC, U&E, CRP (infection, systemic causes)
- 🖥️ MRI spine = gold standard for localisation & cause
- 🖼️ CT spine if bony injury suspected
- 💉 LP + CSF: if infection/inflammatory suspected (TB, MS)
- ⚡ Nerve conduction studies/EMG for chronic or peripheral overlap
🧫 Pathology
- 🔍 Classic “hemisection” syndrome rarely complete in practice-often partial with mixed findings.
💊 Management
- 🫀 Initial trauma care: ABC, IV fluids, spinal immobilisation
- ♿ Rehabilitation: physiotherapy, occupational therapy, long-term neurorehabilitation
- 🚽 Bladder & bowel management; prevent pressure sores
- 🎯 Treat underlying cause:
– Surgery for tumour, disc herniation, abscess
– Antibiotics/antituberculous therapy if infective
– Steroids/DMARDs if inflammatory (e.g. MS)
- 📈 Prognosis: generally better than complete cord injury; ~75% regain functional ambulation if managed appropriately
📌 Exam Pearl:
– Ipsilateral motor & proprioception loss + contralateral pain/temp loss = classic triad.
– Always think of trauma (stab wounds) as the classic cause in exams, but in practice MS and TB are also common.
📚 References
