
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Pupils : Relative Afferent pupillary defect (RAPD)
RAPD can be tested by the swinging torch test to compare the afferent pathway of the pupillary reflex. This test is used to assess the integrity of the afferent limb of the reflex and evaluate retinal and optic nerve function.
Example: Defect in the Right Eye – Swinging Torch Test
- Step 1: Shine a torch in the right eye; due to a defect, there is no pupillary constriction (direct or consensual).
- Step 2: Shine the torch in the left eye; the left pupil constricts directly, and the right pupil constricts consensually.
- Step 3: Shine the torch back in the right eye; the previously constricted pupil now dilates when the light shines.
- This response is called a Marcus Gunn pupil and indicates a relative afferent pupillary defect (RAPD).
- Normal brief oscillations in pupillary size, called hippus, may also occur but should not be mistaken for an afferent defect.
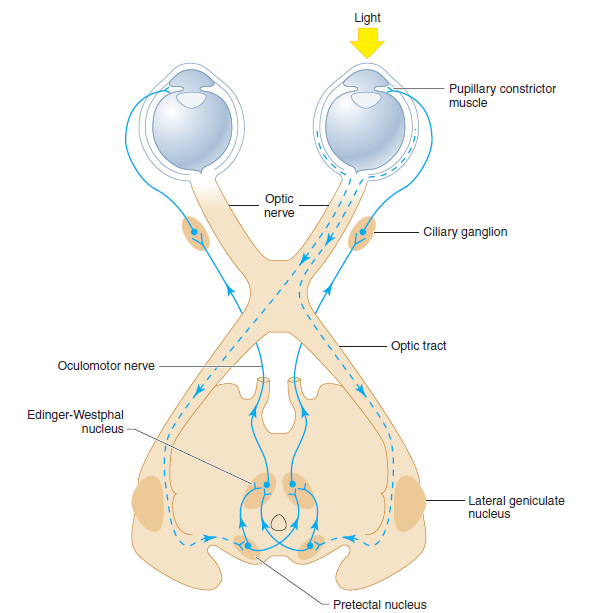
Anatomic basis of the pupillary light reflex. The afferent visual pathways from the retina to the pretectal nuclei of the midbrain are represented by dashed lines and the efferent pupilloconstrictor pathways from the midbrain to the pupillary constrictor muscles by solid lines. Note that illumination of one eye results in bilateral pupillary constriction.
Causes of RAPD
- Optic Neuritis: Often associated with multiple sclerosis, optic neuritis is a common cause of RAPD.
- Ischaemic Optic Neuropathy: Ischaemia in the optic nerve, seen in conditions like giant cell arteritis or anterior ischaemic optic neuropathy (AION).
- Retinal Detachment: Severe retinal detachment can reduce afferent input and lead to RAPD.
- Optic Nerve Compression: Tumours or masses that compress the optic nerve can cause RAPD.
- Glaucoma: Advanced stages can damage the optic nerve and lead to RAPD.
- Severe Retinal Disease: Conditions like central retinal artery occlusion (CRAO) or extensive retinal infarctions.
Diagnosis
- Swinging Flashlight Test: The primary clinical test for detecting RAPD. The examiner moves the light between eyes, with the affected eye showing less pupillary constriction.
- Visual Acuity Testing: Assesses the extent of visual impairment associated with RAPD.
- Color Vision Testing: The Ishihara test can reveal color vision deficiencies linked to optic nerve damage.
- Ophthalmoscopy: Examines the optic nerve head and retina for signs of optic neuritis, retinal detachment, or other conditions.
- Imaging Studies: MRI or CT scans may detect optic nerve lesions, tumours, or structural abnormalities.
Summary
A relative afferent pupillary defect (RAPD) is a clinical sign of asymmetry in sensory input from the optic nerves or retinas. Commonly detected using the swinging flashlight test, RAPD is associated with conditions like optic neuritis, ischaemic optic neuropathy, and retinal detachment. Early diagnosis and treatment of the underlying cause are critical to preserving vision and improving outcomes.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery