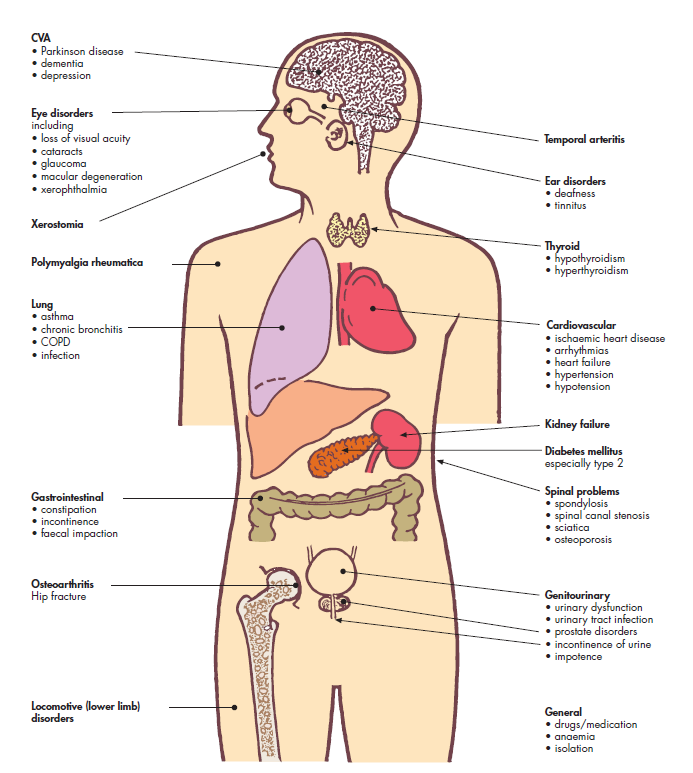
Common Problems in Elderly
👵🧓 Older adults frequently present with complex, overlapping medical conditions.
Ageing is associated with reduced physiological reserve, multimorbidity, polypharmacy, and atypical disease presentation.
As a result, illness often manifests as falls, delirium, immobility, incontinence, or functional decline rather than classic textbook symptoms.
Why Disease Looks Different in the Elderly
- 🔻 Reduced homeostatic reserve → minor insults lead to major deterioration.
- 🧠 Altered pain perception, cognition, and communication.
- 💊 Polypharmacy increases adverse drug events and interactions.
- 🧓 Frailty amplifies vulnerability to acute illness.
- 🏠 Social factors (isolation, carer strain) strongly influence outcomes.
Cardiovascular Conditions
Hypertension
- Driven by arterial stiffening and reduced baroreceptor sensitivity.
- Often asymptomatic yet a major contributor to stroke, heart failure, and vascular dementia.
- Over-aggressive treatment risks postural hypotension, syncope, and falls.
- Targets should be individualised based on frailty and life expectancy.
Ischaemic Heart Disease
- Frequently presents atypically: dyspnoea, fatigue, nausea, delirium.
- Silent myocardial infarction is more common.
- Decision-making around angiography and revascularisation must balance benefit vs burden.
Heart Failure
- HFpEF predominates due to ventricular stiffness and long-standing hypertension.
- Presents with breathlessness, oedema, recurrent admissions, or functional decline.
- Renal dysfunction, hypotension, and frailty often limit guideline-directed therapy.
Atrial Fibrillation
- Prevalence rises sharply with age.
- High embolic stroke risk - anticoagulation usually outweighs fall risk.
- May present with falls, heart failure, or delirium rather than palpitations.
Neurological Conditions
Stroke and TIA
- Incidence and severity increase markedly with age.
- Often complicated by dysphagia, aspiration pneumonia, delirium, and immobility.
- Secondary prevention must consider bleeding risk, cognition, and adherence.
Dementia
- Includes Alzheimer’s disease, vascular dementia, Lewy body dementia, and mixed pathology.
- Progressive decline in memory, executive function, judgement, and daily functioning.
- Vascular risk factors play a major role even in “Alzheimer’s” dementia.
- Behavioural and psychological symptoms (agitation, hallucinations, wandering) often trigger hospital admission.
- Patients are highly vulnerable to delirium, infection, and medication side effects.
- Capacity assessment, safeguarding, and advance care planning are central to management.
- Carer burden and social support often determine outcomes more than cognition alone.
Delirium
- Acute, fluctuating disturbance of attention and awareness.
- Common precipitants: infection, dehydration, pain, constipation, urinary retention, drugs.
- Always represents serious underlying pathology in older adults.
- Strong predictor of mortality, institutionalisation, and future dementia.
Parkinson’s Disease
- Neurodegenerative disorder characterised by bradykinesia, rigidity, tremor, and postural instability.
- Non-motor symptoms (constipation, depression, autonomic dysfunction, hallucinations) often dominate.
- Falls and freezing of gait are major causes of morbidity.
- Medication timing is critical - missed doses can cause severe deterioration.
- Dopaminergic therapy may worsen hallucinations and postural hypotension.
- Advanced disease is associated with dementia, dysphagia, aspiration, and frailty.
Respiratory Conditions
Chronic Obstructive Pulmonary Disease (COPD)
- Cumulative smoking exposure and impaired mucociliary clearance.
- Exacerbations may present with confusion, falls, or reduced mobility.
- Oxygen therapy requires caution due to CO₂ retention risk.
Pneumonia
- Often presents atypically with delirium, anorexia, or immobility.
- Aspiration risk increased by dysphagia and poor cough reflex.
- Mortality is significantly higher than in younger adults.
Endocrine and Metabolic Conditions
Type 2 Diabetes Mellitus
- Insulin resistance and declining beta-cell reserve.
- Hypoglycaemia carries high risk of falls, cognitive impairment, and death.
- Glycaemic targets should prioritise safety over tight control.
Hypothyroidism
- Symptoms overlap with ageing: fatigue, cognitive slowing, weight gain.
- Over-replacement risks atrial fibrillation and osteoporosis.
Osteoporosis
- Often silent until fragility fracture.
- Hip fractures carry high 1-year mortality and loss of independence.
- Vitamin D deficiency and falls risk are key contributors.
Musculoskeletal Conditions
Osteoarthritis
- Degenerative joint disease causing pain, stiffness, and reduced mobility.
- Leads to deconditioning, social isolation, and falls.
- Imaging severity often poorly correlates with symptoms.
Sarcopenia
- Age-related loss of muscle mass and strength.
- Driven by inactivity, inflammation, and malnutrition.
- Central to frailty and poor recovery after illness.
Renal and Urological Conditions
Chronic Kidney Disease
- Physiological decline in GFR with age.
- Marked impact on drug clearance and toxicity.
- AKI often triggered by dehydration or infection.
Benign Prostatic Hyperplasia
- Causes lower urinary tract symptoms, retention, and UTIs.
- Anticholinergic drugs worsen cognition and delirium.
Urinary Incontinence
- Multifactorial: mobility, cognition, bladder dysfunction, medications.
- Strongly associated with falls, depression, and care home admission.
Gastrointestinal and Nutrition
Constipation
- Very common due to immobility, dehydration, and medications.
- Can precipitate delirium, urinary retention, and bowel obstruction.
Malnutrition
- Caused by poor intake, chronic disease, dysphagia, and social isolation.
- Leads to sarcopenia, infection risk, and delayed recovery.
- Unintentional weight loss is always a red flag.
Mental Health
Depression
- Often underdiagnosed and presents atypically.
- May manifest as apathy, weight loss, or somatic complaints.
- Treating depression improves functional outcomes.
Geriatric Syndromes (Cross-Cutting)
- 🚶 Falls: usually multifactorial (vision, balance, drugs, environment).
- 🧓 Frailty: reduced resilience to stressors; predicts poor outcomes.
- 💊 Polypharmacy: increases delirium, falls, and hospitalisation.
- 🛏️ Pressure ulcers: marker of immobility and poor overall health.
Key Take-Home Principles
- Think in syndromes, not single diagnoses.
- Expect atypical presentations.
- Function, cognition, and goals of care matter as much as pathology.
- Small insults can cause disproportionate decline.
- Comprehensive Geriatric Assessment is central to good care.
