| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Trigeminal Nerve (Vth Nerve)
Related Subjects: |Olfactory Nerve |Optic Nerve |Oculomotor Nerve |Trochlear Nerve |Trigeminal Nerve |Abducent Nerve |Facial Nerve |Vestibulocochlear Nerve |Glossopharyngeal Nerve |Vagus Nerve |Accessory Nerve |Hypoglossal Nerve
The trigeminal nerve (CN V) is the largest cranial nerve. It carries both sensory and motor fibres, providing facial sensation and controlling muscles of mastication. It arises from the pons and is associated with the first pharyngeal arch.
🔎 Anatomy & Course
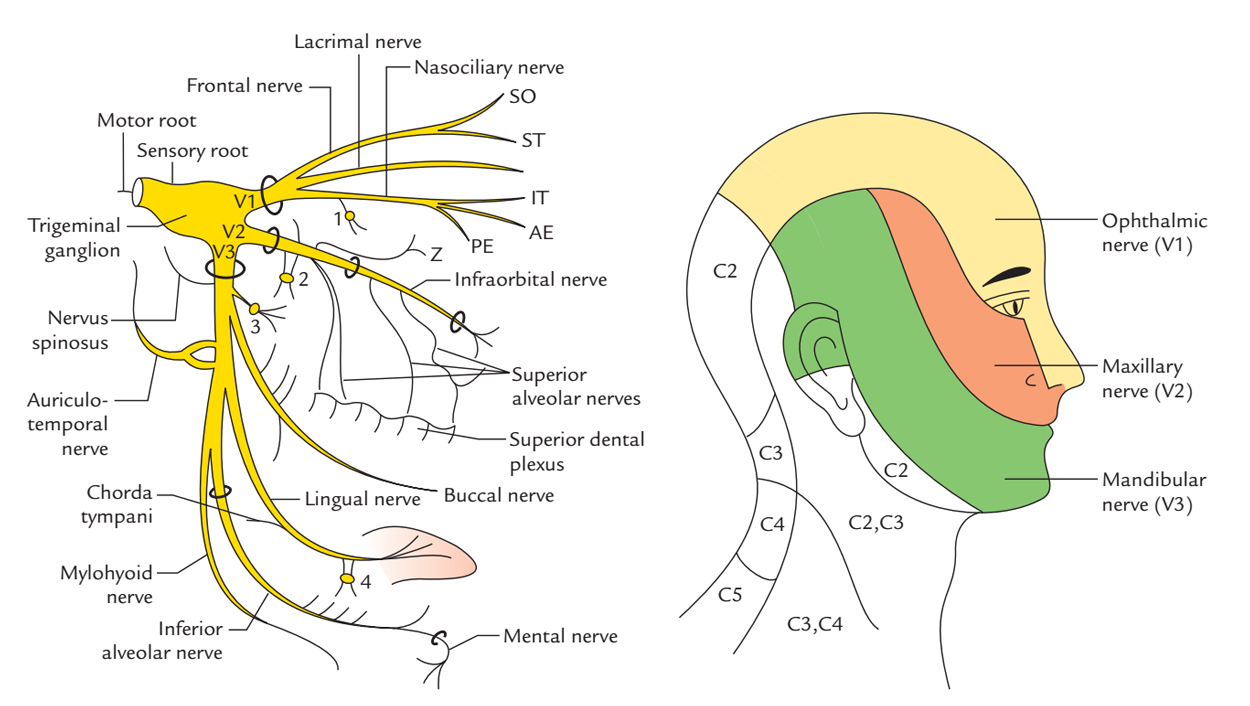
- Origin: Emerges from the pons with a large sensory root and a smaller motor root.
- Trigeminal (Gasserian) Ganglion: Located in Meckel’s cave; contains sensory neuron cell bodies.
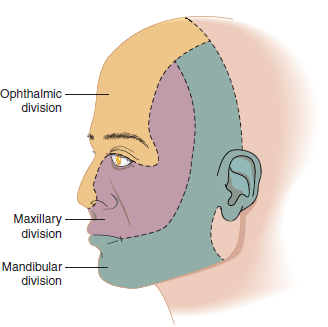
- Divisions: From the ganglion, divides into three major branches: ophthalmic (V1), maxillary (V2), mandibular (V3).
🧩 Branches & Functions
| Branch | Type | Key Areas Supplied | Clinical Notes |
|---|---|---|---|
| Ophthalmic (V1) | Sensory | Forehead, scalp, upper eyelid, cornea, dorsum of nose | Herpes zoster ophthalmicus can threaten vision. Afferent limb of corneal reflex. |
| Maxillary (V2) | Sensory | Lower eyelid, cheek, upper lip, upper teeth & gums, nasal mucosa, palate | Dental blocks often target infraorbital or superior alveolar branches. |
| Mandibular (V3) | Mixed |
Sensory: lower lip, chin, lower teeth & gums, anterior 2/3 tongue (general sensation only), external ear Motor: muscles of mastication, mylohyoid, anterior digastric, tensor tympani, tensor veli palatini |
Jaw deviates towards side of lesion due to unopposed pterygoid action. |
⚡ Functions
- Sensory: Touch, pain, temperature from face, oral and nasal cavities, teeth, anterior 2/3 tongue.
- Motor: Chewing, swallowing support, dampening loud sounds (tensor tympani).
🩺 Clinical Relevance
- Trigeminal Neuralgia: Severe, stabbing facial pain. Treated with carbamazepine, nerve blocks, or microvascular decompression.
- Lesions: Trauma, tumours, MS, or infections may cause sensory loss and weak mastication.
- Corneal Reflex: Afferent: V1; Efferent: facial nerve (orbicularis oculi).
- Dental Anaesthesia: Inferior alveolar nerve block (V3) for mandibular teeth; infraorbital/maxillary nerve blocks for upper teeth.
🧪 Diagnostic Evaluation
- Examination: Test light touch, pinprick, and temperature across V1–V3 dermatomes; palpate masseter/temporalis while patient clenches teeth.
- Imaging: MRI for tumours, vascular compression, or demyelination; CT for fractures.
- Electrophysiology: Nerve conduction and evoked potentials to assess function.
🧠 Trigeminal Nerve (CN V) Palsy – Causes & Management
A trigeminal nerve palsy causes facial sensory loss (V1 ophthalmic, V2 maxillary, V3 mandibular) ± weakness of mastication (V3 motor root). The trigeminal nerve has a large sensory root entering the pons and a motor root supplying muscles of mastication. Lesions may occur anywhere from the brainstem nuclei to the peripheral branches, so localisation is critical.
| Cause 🧩 | Typical Features 🔍 | Immediate Management 🚑 | Definitive / Ongoing Management 🏥 |
|---|---|---|---|
| Brainstem stroke 🧠 | Facial sensory loss ± contralateral body deficits (crossed signs) | Activate stroke pathway | Secondary stroke prevention |
| Multiple sclerosis 🔥 | Young patient; sensory loss or trigeminal neuralgia | MRI brain with contrast | Steroids for relapse; disease-modifying therapy |
| Cerebellopontine angle tumour 🎗️ | Gradual facial numbness ± hearing loss (VIII involvement) | MRI brain | Neurosurgical / oncology referral |
| Cavernous sinus lesion 🧠 | V1/V2 sensory loss + III, IV, VI palsies | Urgent MRI ± MRV | Treat thrombosis, tumour, or infection |
| Herpes zoster (Ramsay Hunt / zoster ophthalmicus) 🦠 | Painful vesicular rash in dermatomal distribution | Start antivirals urgently (within 72h) | Analgesia; ophthalmology if V1 involved |
| Skull base tumour or metastasis 🦴 | Progressive numbness; multiple cranial nerves | MRI skull base | Oncology management |
| Trauma 🚗 | Facial fractures; sensory deficit in specific branch | CT facial bones | Maxillofacial management |
| Iatrogenic (dental procedures) 🦷 | Isolated V2 or V3 numbness post-procedure | Clinical assessment | Observation or specialist referral |
| Perineural tumour spread 🎗️ | Gradual sensory loss; history of skin cancer | MRI with contrast | Oncological management |
| Idiopathic trigeminal neuropathy ❓ | Isolated sensory loss; no cause found | Exclude structural pathology | Observation ± neuropathic pain control |
⚡ Practical Approach
Localisation depends on pattern: isolated V1 involvement suggests orbital or cavernous sinus pathology; involvement of all divisions suggests root or ganglion lesion; crossed sensory signs indicate brainstem disease. Motor involvement (jaw deviation toward lesion, weak mastication) implies V3 root damage. Always image new unexplained trigeminal sensory loss, particularly if progressive.
📌 OSCE Exam Tips
- Always compare sides when testing sensation.
- Corneal reflex: loss on one side suggests V1 or VII lesion.
- Jaw deviation: towards the weak side (ipsilateral V3 lesion).
- Remember: sensation at angle of mandible = cervical plexus (C2), not CN V.
📚 References
- Standring S. Gray's Anatomy, 41st ed. Elsevier, 2016.
- Bear MF et al. Neuroscience: Exploring the Brain, 4th ed. Wolters Kluwer, 2015.
- Levin KH. Cranial Neuropathies. Semin Neurol. 2009;29(1):38-44.
🖼️ Visuals
Dermatome maps of V1, V2, V3 are invaluable for learning. Example resources:
{kind=link}