
🧠 Brain MRI Basics
Magnetic Resonance Imaging (MRI) is an advanced, non-ionizing imaging technique that provides highly detailed images of the brain and spinal cord. Unlike CT, which is largely limited to axial views, MRI can image in any plane (axial, sagittal, coronal), making it invaluable in neuroimaging.
- Uses radio waves + magnetic fields (no radiation ☢️).
- Signal depends on hydrogen atoms and tissue relaxation times (T1, T2), not electron density (as in CT).
- Excellent soft-tissue contrast → gold standard for CNS pathology.
⚙️ How MRI Works
- Hydrogen nuclei alignment: Protons align in strong magnetic field → net magnetization.
- Larmor frequency: Radiofrequency pulses excite protons; when relaxed, they emit measurable signals.
- Spin echo & Fourier transform: Signals are reconstructed into high-resolution images.
⚠️ Limitations & Contraindications
Typical scan time: 10–30 mins. Narrow, noisy scanner → difficult for claustrophobic patients.
| Contraindications 🚫 |
|---|
|
🎯 Key MRI Sequences
- T1WI: Anatomy 🏗️; fat bright, CSF dark. Useful for structural details & gadolinium enhancement.
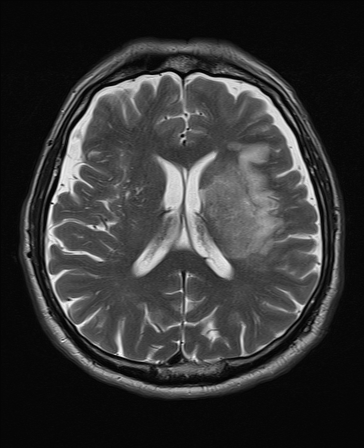
- T2WI: Pathology 🔦; CSF/edema bright. Sensitive to tumours, inflammation, demyelination.
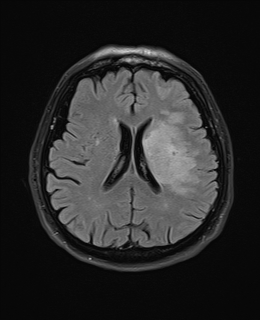
- FLAIR: T2 variant suppressing CSF; highlights periventricular lesions (e.g. MS).
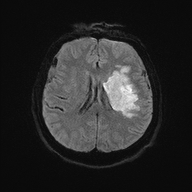
- DWI: Stroke sequence ⚡; detects restricted diffusion within minutes.
- ADC maps: Confirm true restriction vs T2 shine-through.
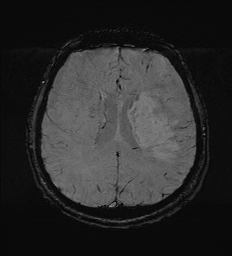
- GRE/SWI: Blood 🩸 & iron; detects microbleeds, calcification, cavernomas.
💉 Gadolinium Contrast
- Highlights breakdown of blood–brain barrier (tumours, abscesses, MS plaques).
- Risk: nephrogenic systemic fibrosis in CKD (eGFR <30) → use only if essential.
🧾 Common Indications
- Stroke: DWI = most sensitive; FLAIR = chronic lesions.
- Tumours: MRI + gadolinium = precise margins & infiltration.
- MS: Periventricular “Dawson’s fingers” best seen on FLAIR.
- Dementia: Hippocampal atrophy (AD), frontotemporal atrophy (FTD).
- Infections: Abscess vs cyst; DWI helpful.
- Spinal cord disease: MS plaques, compression, tumours.
🖼️ Example Sequences
| T2 FLAIR | T2 |
|---|---|
 |
 |
| DWI | ADC |
 |
 |
| SWI | T1 Sagittal |
 |
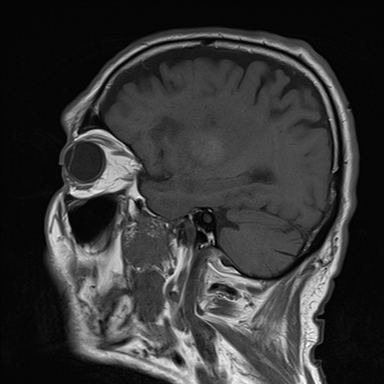 |
🚑 CT vs MRI: Quick Comparison
| Feature | CT | MRI |
|---|---|---|
| Speed | ✅ Fast (emergency stroke, trauma) | ⏳ Slower (10–30 min) |
| Radiation | ☢️ Yes | 🚫 No |
| Best for | Bone, acute haemorrhage, trauma | Soft tissues, tumours, demyelination, stroke (DWI) |
| Stroke (acute) | Excludes bleed | Detects infarct early ⚡ |
📑 MRI Sequences Cheat-Sheet
| Sequence | What’s Bright ✨ | What’s Dark ⚫ | Main Uses 🎯 |
|---|---|---|---|
| T1-Weighted (T1WI) | Fat, subacute haemorrhage, gadolinium contrast | CSF, edema | Anatomy, post-contrast enhancement, haemorrhage staging |
| T2-Weighted (T2WI) | CSF, edema, demyelination, most pathology | Fat, calcification, acute haemorrhage | Pathology detection (tumours, inflammation, MS plaques) |
| FLAIR | Edema, gliosis, demyelination near CSF spaces | CSF (suppressed), normal fluid | MS, periventricular lesions, subarachnoid space pathologies |
| DWI (Diffusion-Weighted) | Restricted water diffusion (acute stroke, abscess) | Normal brain tissue, vasogenic edema | Hyperacute stroke ⚡, abscess vs cyst, encephalitis |
| ADC Map | Normal diffusion (bright) | Restricted diffusion (dark in stroke) | Confirms true restriction (differentiate stroke vs T2 shine-through) |
| SWI / GRE | Calcification, veins | Blood products, iron, microbleeds | Haemorrhage 🩸, cavernomas, traumatic brain injury, neurodegeneration |
🧠 Exam Tip: “Bright on T2, pathology true” - most pathologies are hyperintense on T2. Always check DWI + ADC for stroke.
✅ Conclusion
MRI is indispensable in neuroimaging - unrivalled for CNS detail, guiding diagnosis and management of stroke, tumours, infections, MS, dementia, and spinal disease. With its range of sequences and contrast options, it provides both structural and functional insights, shaping modern neurology and neurosurgery practice.