Related Subjects:
|Thunderclap Headache
|Subarachnoid Haemorrhage
|Perimesencephalic Subarachnoid haemorrhage
|Haemorrhagic stroke
|Cerebellar Haemorrhage
|Putaminal Haemorrhage
|Thalamic Haemorrhage
|ICH Classification and Severity Scores
|Saccular aneurysms
🧠 Perimesencephalic Subarachnoid Haemorrhage (PM-SAH) is a subtype of SAH localised around the midbrain without aneurysm or vascular malformation.
Represents 15–20% of all SAH cases and carries a significantly better prognosis than aneurysmal SAH (aSAH).
📌 Etiology & Pathophysiology
- Non-aneurysmal bleeding: Distinguishes PM-SAH from aneurysmal SAH.
- Venous bleeding hypothesis: Rupture of small perimesencephalic veins → localised blood accumulation.
- Potential triggers: Minor trauma, Valsalva manoeuvres, acute rises in intracranial venous pressure.
- Prognosis: Very low risk of rebleeding; long-term outcomes favourable.
- Pathophysiology: Localised subarachnoid blood without significant vasospasm or ICP elevation in most cases.
🩺 Clinical Presentation
- Sudden, severe “thunderclap” headache, often occipital or retro-orbital 🌩️.
- Mild neurological signs: meningism, photophobia, occasional cranial nerve deficits.
- Other: nausea, vomiting, transient loss of consciousness.
- Typical patient: middle-aged, slight male predominance.
⚠️ Risk Factors
- Hypertension 🩸
- Middle age
- Male sex ♂️
- Smoking 🚬, alcohol 🍺
- Rare genetic predisposition
🔬 Investigations
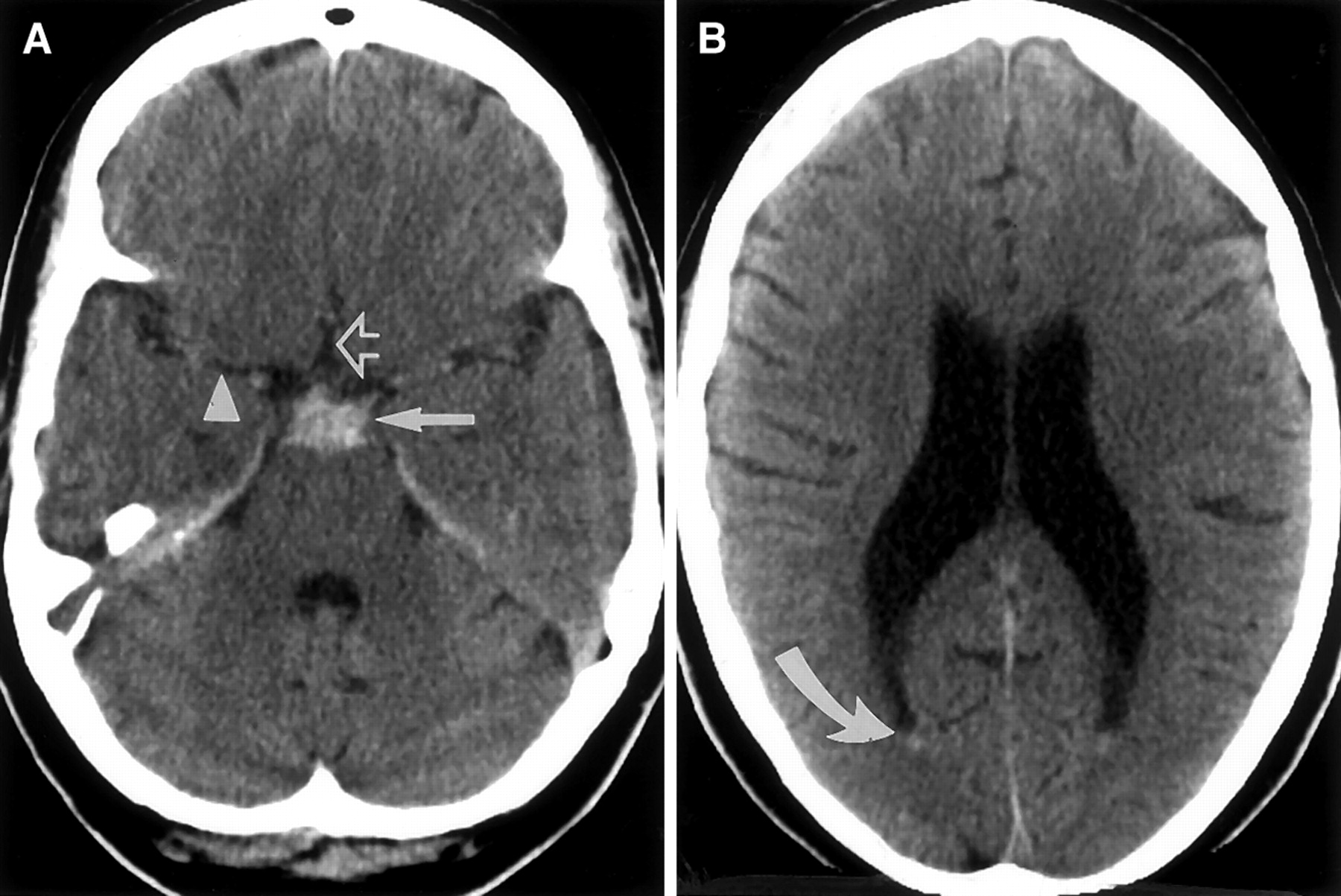
- CT head: Blood around perimesencephalic cisterns; first-line, rapid.
- MRI brain: More sensitive for small or subtle bleeds (FLAIR, SWI sequences).
- CTA / DSA: Exclude aneurysm or vascular malformation (diagnosis of exclusion).
- LP: Consider if CT negative but clinical suspicion persists; xanthochromia confirms SAH.
- Bloods: FBC, U&E, coagulation profile, platelets.
🧾 Diagnostic Criteria
- Sudden severe thunderclap headache ± mild neuro signs.
- CT/MRI shows blood confined to perimesencephalic cisterns.
- No aneurysm or vascular malformation on CTA/DSA.
- Absence of poor prognostic features (massive bleed, hydrocephalus, severe vasospasm).
🔍 Differential Diagnosis
- Aneurysmal SAH (aSAH) – requires urgent neurosurgical input.
- Reversible cerebral vasoconstriction syndrome (RCVS) – recurrent thunderclap headaches.
- Intracerebral haemorrhage (ICH).
- Migraine with aura / sudden-onset migraine.
- Intracranial hypotension (spontaneous or post-LP).
- Meningitis / encephalitis (if systemic signs present).
💊 Management
- Initial: ABC stabilization, analgesia, hospital admission for observation.
- Monitoring: Neurological observations, BP control (SBP <160 mmHg), hydration.
- Hydrocephalus: Rare; if present → consider external ventricular drain (EVD) or lumbar drainage.
- Follow-up imaging: Repeat CTA/DSA to exclude delayed aneurysms.
- Rehabilitation: Support for residual cognitive or motor deficits.
- Patient education: Reassure about benign course compared to aneurysmal SAH, advise on warning signs.
📈 Prognosis
- Generally benign course; mortality much lower than aneurysmal SAH.
- Most patients achieve full recovery with minimal or no neurological deficit.
- Rebleeding and clinically significant vasospasm are extremely rare.
- Excellent long-term quality of life in survivors.
⚠️ Complications
- Hydrocephalus (early, rare)
- Seizures (rare)
- Infections (if invasive monitoring/drains used)
- Electrolyte disturbances (stress-related)
- Psychological sequelae – anxiety, PTSD, post-SAH headache syndromes
📝 Exam / Student Tips
- 💡 PM-SAH is a benign SAH subtype; differentiate from aneurysmal SAH to avoid unnecessary surgery.
- 🔍 Look for blood limited to perimesencephalic cisterns on imaging.
- 🩺 Mild neuro features with sudden thunderclap headache = classic presentation.
- 📆 Repeat vascular imaging recommended to exclude delayed aneurysm detection.
- ⚠️ Red flags: worsening headache, focal deficits, hydrocephalus → escalate to neurosurgery.
📚 References
- van Gijn & Rinkel. Subarachnoid haemorrhage: diagnosis & management. Brain 2001.
- Feigin VL et al. (2023). Global burden of stroke & SAH. Stroke, 54(3).
- Sanchez-Moreno J et al. (2022). PM-SAH: a systematic review. Neurol Res Pract, 4(1).
- Mohr FW et al. (2021). Outcome after PM-SAH: meta-analysis. Neurosurg Rev, 44(4).
- Kim DW et al. (2020). Management of non-aneurysmal PM-SAH. J Stroke Cerebrovasc Dis, 29(8).
