
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Nose
Related Subjects: |AP of the Oesophagus |AP of the Diaphragm |AP of the Large Bowel (Colon, Rectum, Anal Canal) |AP of Small Bowel |AP of the Biliary system |AP of the Bone Marrow |AP of the Eye |AP of the Pharynx |AP of the Larynx |AP of the Ear |AP of the Nose |AP of Male Genitalia |AP of the Breast |AP of the Stomach |AP of the Rectum |AP of the Spleen
👂👃👄 The nose is the entrance to the upper airway and a specialised sensory organ for olfaction. Its core functions are to condition inspired air (warm, humidify, filter), provide airflow resistance that supports normal breathing mechanics, enable smell, contribute to speech resonance, and support mucosal immunity. Clinically, nasal anatomy explains common problems like rhinitis, sinusitis, epistaxis, septal deviation, and CSF rhinorrhoea.
1) Gross Anatomy
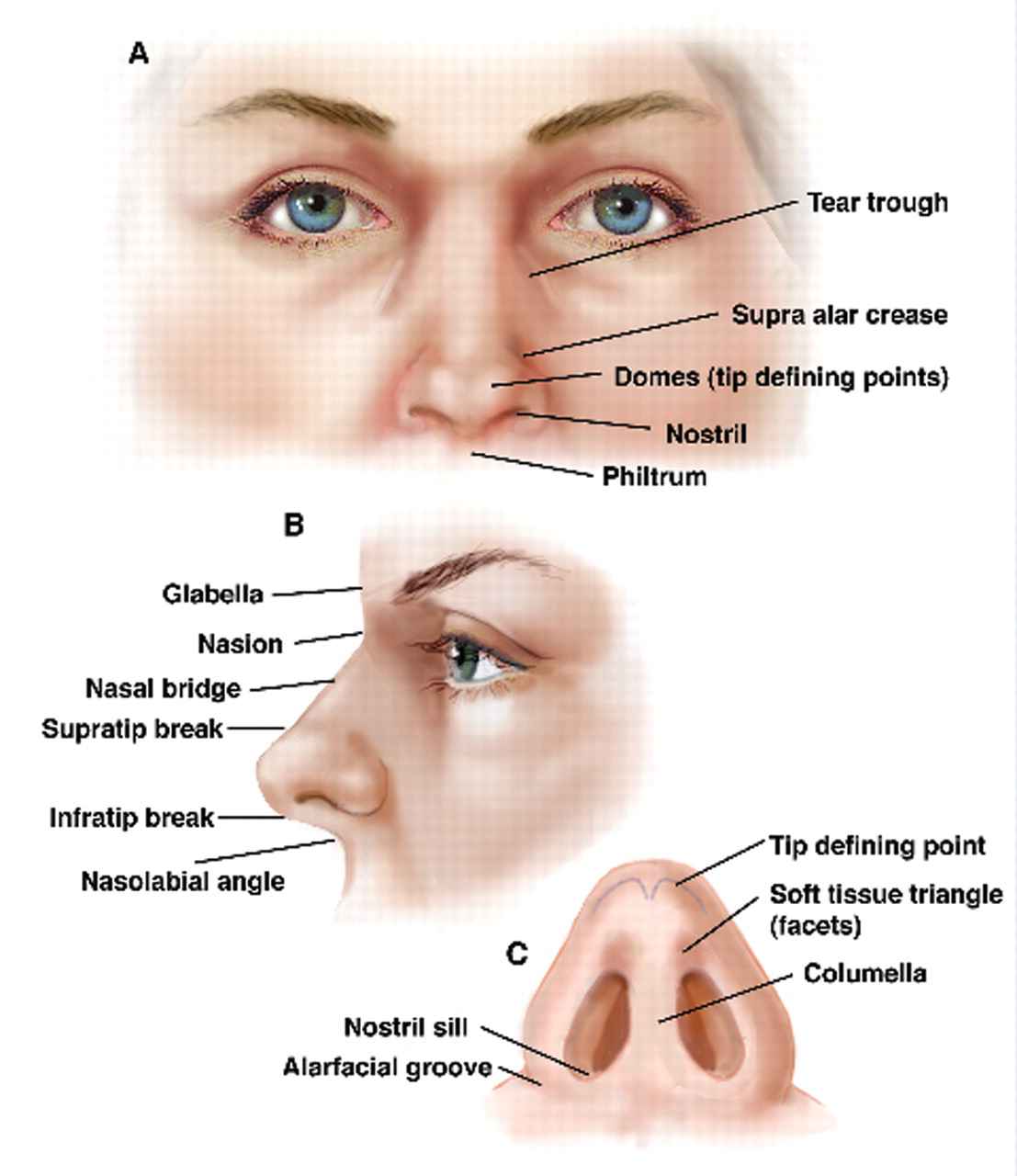
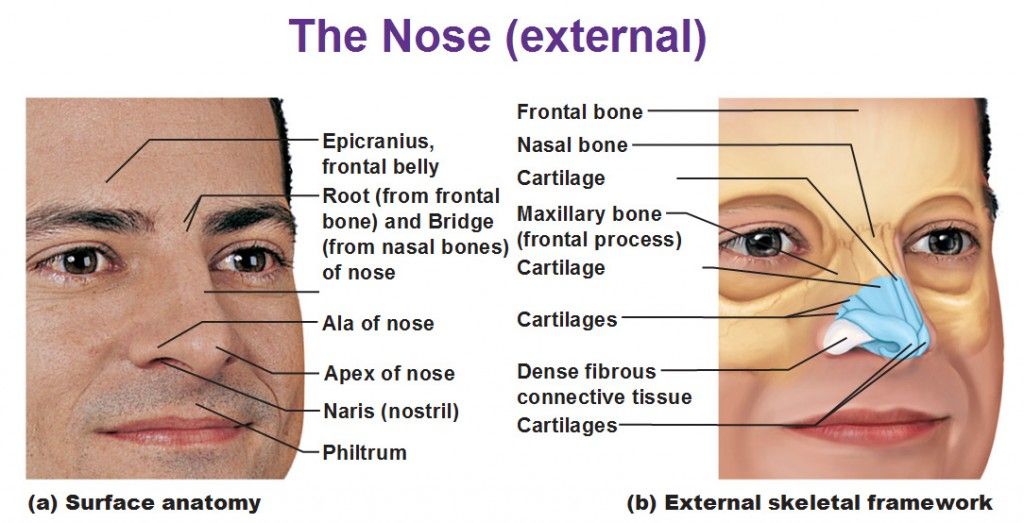
🌐 A) External Nose
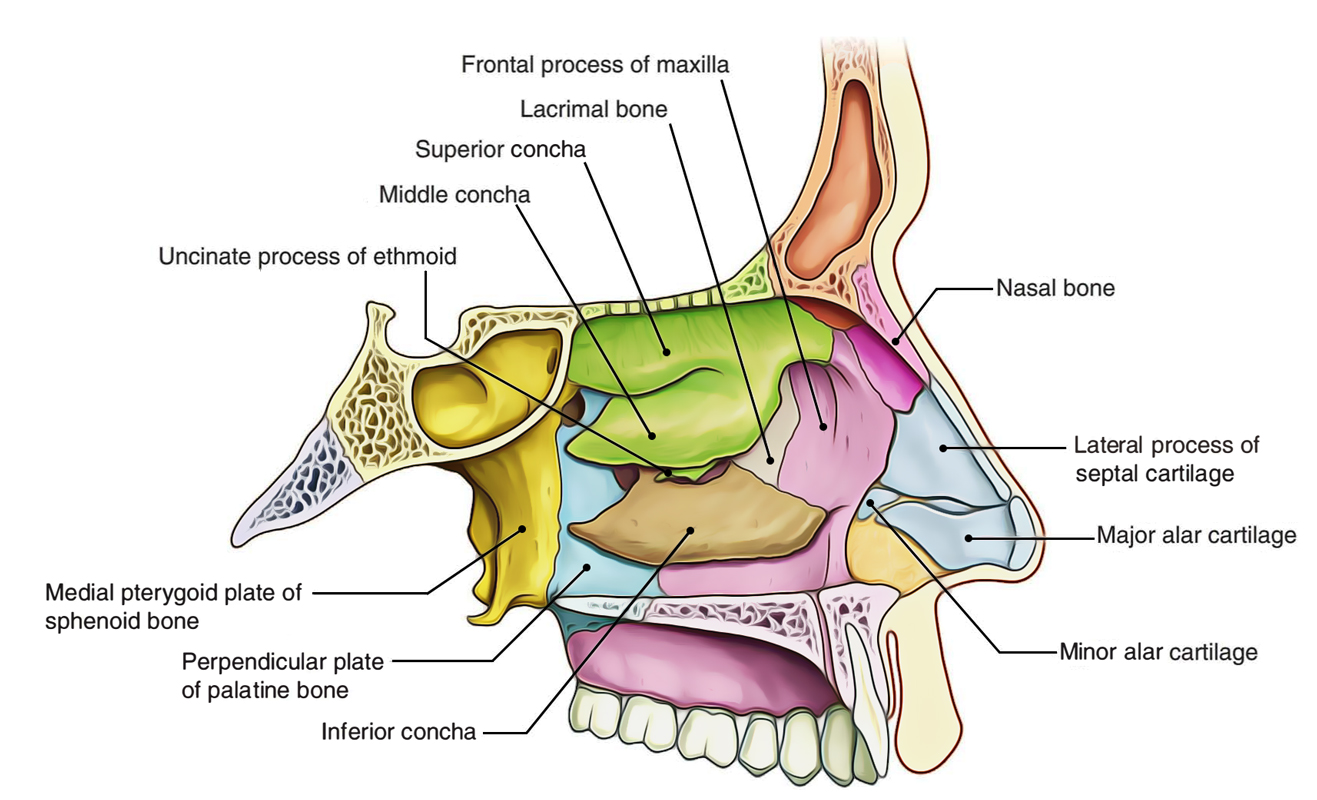
- Bony framework: nasal bones + frontal processes of maxilla (upper third).
- Cartilaginous framework: septal cartilage, lateral nasal cartilages, alar cartilages (lower two-thirds).
- Nares (nostrils): openings to nasal vestibule; lined by skin with vibrissae (coarse hairs) for particulate filtration.
- Clinical: nasal fractures can cause deformity and obstruction; always consider septal haematoma (cartilage necrosis risk if missed).
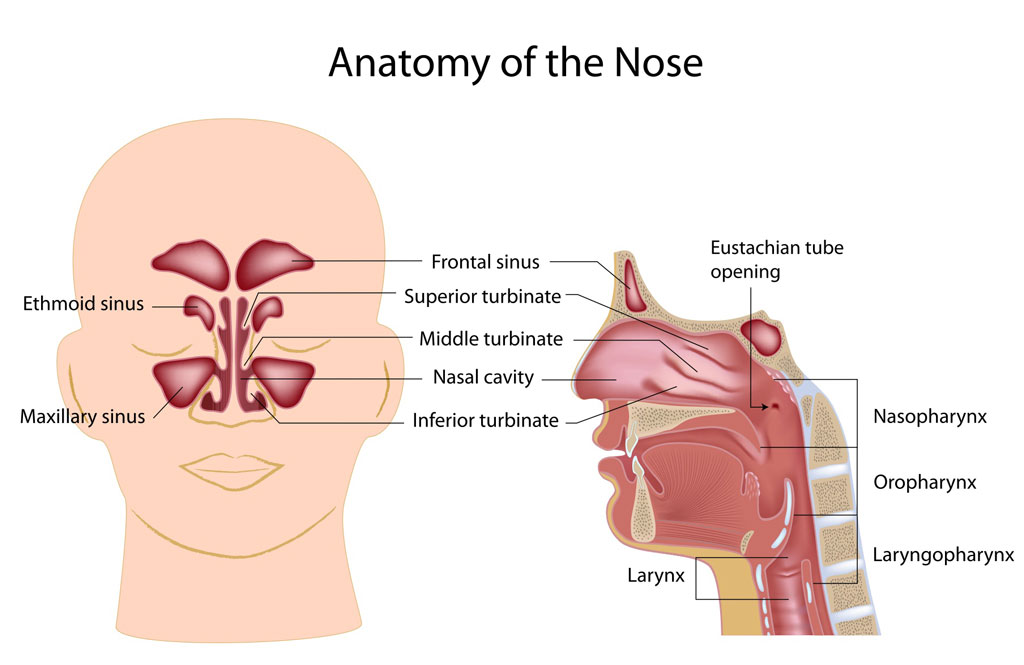
🏠 B) Nasal Cavity (Internal Nose)
The nasal cavity runs from the nares to the choanae (posterior nasal apertures) opening into the nasopharynx. It is divided by the nasal septum and shaped by the turbinates, creating turbulent airflow that maximises contact between air and mucosa for effective conditioning.
- Boundaries:
- Floor: hard palate (maxilla + palatine bones) - separates nose from oral cavity.
- Roof: nasal bones anteriorly; cribriform plate of ethmoid centrally; sphenoid posteriorly.
- Medial wall: nasal septum.
- Lateral wall: conchae (turbinates) and meatuses (drainage pathways).
- Nasal septum:
- Cartilaginous (anterior): septal cartilage.
- Bony (posterior): perpendicular plate of ethmoid + vomer.
- Covered by vascular mucosa; anterior septum is a common bleeding site.
- Clinical: deviation can cause unilateral obstruction, snoring, recurrent epistaxis; septal perforation can cause whistling/crusting.
- Nasal conchae (turbinates): superior, middle (ethmoid), and inferior (separate bone)
- Function: increase surface area and create airflow turbulence → warming, humidification, filtration.
- Inferior turbinate is often most clinically relevant for congestion and hypertrophy.
- Clinical: turbinate hypertrophy is common in allergic rhinitis; decongestants shrink mucosa by vasoconstriction.
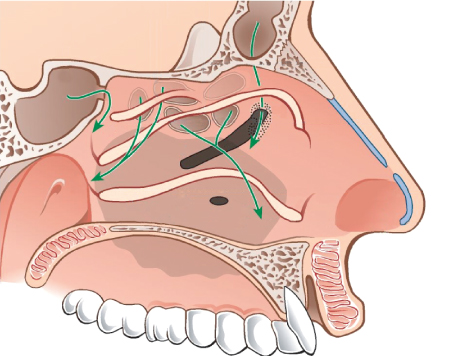
- Meatuses (drainage channels beneath conchae):
- Inferior meatus: receives the nasolacrimal duct → explains runny nose with crying.
- Middle meatus: key drainage zone (ostiomeatal complex):
- frontal sinus (via frontonasal duct)
- maxillary sinus
- anterior ethmoidal air cells
- Superior meatus: drains posterior ethmoids.
- Sphenoethmoidal recess: drains sphenoid sinus.
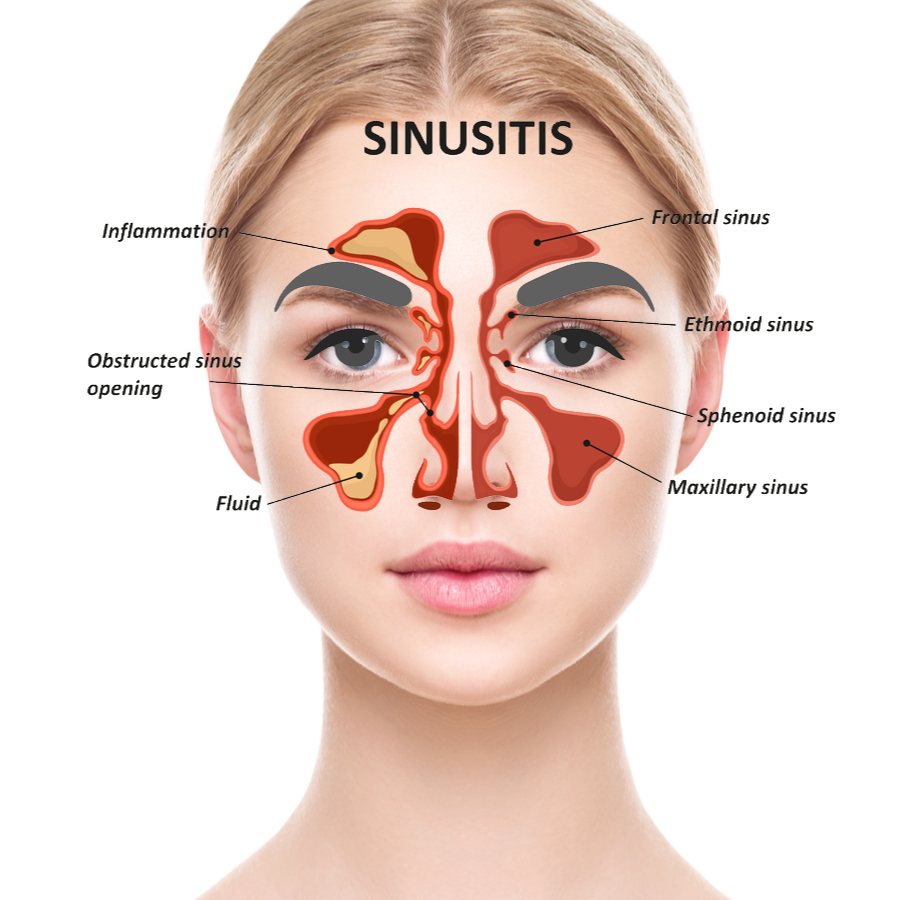
🌀 C) Paranasal Sinuses
Paranasal sinuses are air-filled cavities lined with respiratory mucosa. They lighten the skull, contribute to voice resonance, and produce mucus that drains into the nasal cavity. Impaired drainage and mucociliary dysfunction are central to sinusitis pathophysiology.
- 🟩 Maxillary sinuses: largest; drain into middle meatus.
📌 Exam tip: maxillary sinus ostium sits relatively high → drainage can be poor when inflamed. - 🟦 Frontal sinuses: drain via frontonasal duct to middle meatus; pain often forehead.
- 🟨 Ethmoid air cells: multiple small cells; drain to superior/middle meatus depending on group; can cause medial orbital pain.
- 🟥 Sphenoid sinus: drains to sphenoethmoidal recess; close to optic nerve, cavernous sinus, and pituitary.
📌 Clinical: surgical access route for trans-sphenoidal pituitary procedures.
2) Microanatomy and Mucosa
- Nasal vestibule: skin with hair follicles and sebaceous glands (front-line particulate filtration).
- Respiratory mucosa: ciliated pseudostratified columnar epithelium with goblet cells.
- Mucociliary clearance: mucus traps particles; cilia move mucus posteriorly to nasopharynx for swallowing.
- Clinical: viral infections, smoking, and dehydration impair clearance → congestion and sinusitis risk.
- Olfactory mucosa: located high in nasal cavity (roof, superior septum, superior turbinate region).
- Contains olfactory receptor neurons whose axons pass through cribriform plate → olfactory bulb.
- Clinical: head trauma can shear fibres → anosmia and risk of CSF leak.
3) Blood Supply and Epistaxis 🩸
The nasal cavity has one of the richest arterial supplies in the body, supporting rapid warming of inspired air. This vascularity also explains why epistaxis is common-especially from Little’s area (Kiesselbach’s plexus) on the anterior septum.
- Kiesselbach’s plexus (Little’s area): anterior septal anastomosis → most common site of nosebleeds.
- Arterial contributors: branches of facial, maxillary, and ophthalmic arteries.
- Posterior epistaxis: often from sphenopalatine artery territory → heavier bleeding, harder to control, may require posterior packing or cautery/embolisation.
4) Innervation
- Olfaction: CN I (olfactory) via olfactory mucosa → olfactory bulb.
- General sensation:
- V1 (ophthalmic division): anterosuperior nasal cavity (anterior ethmoidal nerve).
- V2 (maxillary division): posteroinferior nasal cavity (nasopalatine and posterior nasal nerves).
- Autonomic control:
- Parasympathetic: increases glandular secretion (watery rhinorrhoea).
- Sympathetic: vasoconstriction reduces mucosal swelling (basis of topical decongestants).
5) Physiology
🌬️ A) Air Conditioning: Warming, Humidifying, Filtering
- Warming: dense vascular plexuses transfer heat rapidly to inspired air.
- Humidification: mucosa adds water vapour; helps protect lower airways from drying and irritation.
- Filtration: vibrissae + mucus trap particles; cilia clear debris posteriorly.
- Airflow resistance: nasal passages provide physiologic resistance that supports efficient ventilation dynamics.
🧠 B) Olfaction (Smell)
- Odorants dissolve in mucus → bind receptors on olfactory neurons → signals to olfactory bulb and cortex.
- Smell contributes heavily to flavour; nasal obstruction often causes “loss of taste” perception.
🎶 C) Resonance and Speech
- The nose and sinuses influence voice resonance; nasal obstruction can cause hyponasal speech, while velopharyngeal dysfunction can cause hypernasality.
🛡️ D) Immune Defence
- Mucus and cilia are part of innate defence; mucosa also contains immune cells and IgA contributing to pathogen neutralisation.
⚠️ Clinical Correlations (High Yield)
- Rhinitis: allergic/viral → mucosal oedema, turbinate hypertrophy, rhinorrhoea; allergic rhinitis often itchy with sneezing.
- Sinusitis: typically follows ostiomeatal obstruction; facial pain/pressure patterns relate to affected sinus.
- Epistaxis: anterior (Little’s area) common; posterior bleeds more severe.
- Septal haematoma: post-trauma emergency → cartilage necrosis if not drained.
- CSF rhinorrhoea: clear unilateral watery discharge after head trauma; risk of meningitis (cribriform plate region).
- Nasal polyps: chronic inflammation; can cause anosmia and obstruction; associated with asthma/aspirin sensitivity in some patients.
🌟 Key Points for Students
- Nasal conchae = ↑ surface area and turbulence for air conditioning 🌬️.
- Middle meatus/ostiomeatal complex = drainage hub for most sinuses (sinusitis favourite).
- Little’s area = commonest epistaxis site 🩸.
- Sphenoid sinus sits near pituitary/optic nerve → deep complications and surgical relevance 🧠.
✅ Conclusion
The nose is a multifunctional organ integrating air conditioning, filtration, olfaction, and resonance. Its turbinates and mucosa maximise airflow–mucosa contact, while rich vascular supply enables rapid warming but predisposes to epistaxis. Understanding drainage pathways (especially the middle meatus) and key danger areas (cribriform plate, posterior epistaxis) is essential for ENT and acute care practice.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery