
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
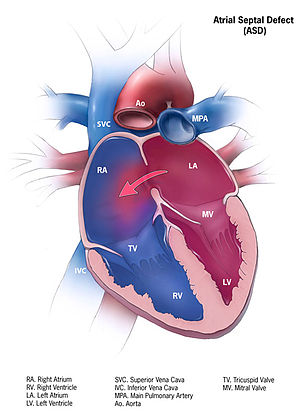
Atrial septal defect (ASD) ✅
Related Subjects: |Congenital Acyanotic Heart Disease |Congenital Cyanotic Heart Disease |Cardiac Embryology |Cyanosis - Central and Peripheral |Down's syndrome (Trisomy 21) |Tetralogy of Fallot |Patent Foramen Ovale (PFO) |Ventricular Septal defect (VSD) |Atrial Septal defect (ASD) |Ebstein anomaly |Eisenmenger's syndrome
🫀 In atrial septal defect (ASD), the murmur is not caused by blood flowing across the septal defect itself, but by increased flow across the pulmonary valve, producing an ejection systolic murmur at the left upper sternal edge. 🔊 Fixed wide splitting of S2 is a classic hallmark. 🧪 Closure is usually considered when there is a haemodynamically significant left-to-right shunt causing right-heart enlargement, often supported by a Qp:Qs ratio >1.5:1, provided pulmonary vascular disease is not irreversible. 💉 Routine infective endocarditis prophylaxis is not recommended for dental procedures under NICE guidance.
📖 About
- ASD is a congenital defect with an abnormal communication between the atria, causing a left-to-right shunt.
- This leads to right atrial (RA) and right ventricular (RV) volume overload and increased pulmonary blood flow.
- ASD accounts for an important proportion of congenital heart disease and is more commonly recognised in females.
- ⚠️ The strongest syndrome association is not with all ASDs equally: ostium primum ASD / partial AV septal defect has a particularly important association with Down syndrome.
⚙️ Pathophysiology
- ⬅️ Oxygenated blood flows from the left atrium to the right atrium because left-sided pressures are higher.
- 🫀 This causes chronic right-sided volume loading, leading to RA and RV dilatation over time.
- 🫁 Pulmonary blood flow increases, which may eventually contribute to pulmonary vascular remodelling in longstanding large unrepaired defects.
- ⚠️ If pulmonary vascular disease becomes severe and irreversible, Eisenmenger physiology may develop, with shunt reversal and cyanosis.
🔎 Types of ASD
- Ostium secundum: the commonest true ASD, located in the region of the fossa ovalis.
- Ostium primum: located low in the atrial septum near the AV valves; this is better thought of as part of the atrioventricular septal defect (AVSD) spectrum and may be associated with AV valve regurgitation.
- Sinus venosus defect: near the SVC or IVC junction; often associated with partial anomalous pulmonary venous drainage.
- Unroofed coronary sinus: rare communication involving the coronary sinus and left atrium.
🩺 Clinical Presentation
- 👶 Many children are asymptomatic, especially with small defects.
- 🧒 Larger defects may present with poor weight gain, exercise intolerance, or recurrent respiratory symptoms in childhood.
- 🧑 Symptoms later in life include:
- 🌬️ exertional dyspnoea
- 😴 fatigue
- 💓 palpitations due to atrial arrhythmias
- 🧠 rarely paradoxical embolic events such as stroke
- Examination:
- 🌟 Fixed wide split S2
- 🎧 Ejection systolic murmur at the left upper sternal edge due to increased pulmonary flow
- 🎵 A low-pitched mid-diastolic murmur at the lower sternal border may occur with large shunts due to increased tricuspid flow
- 🫀 A parasternal heave may reflect RV volume loading
- Advanced disease: signs of right heart failure, pulmonary hypertension, or cyanosis if Eisenmenger physiology develops.
🧪 Investigations
- ECG:
- Secundum ASD may show right axis deviation, RV volume-loading changes, or incomplete RBBB.
- Primum defects more classically show left axis deviation and may have first-degree AV block.
- Chest X-ray: may show cardiomegaly, right heart enlargement, and pulmonary plethora in significant shunts.
- Transthoracic echocardiography: the key first-line test; confirms the defect, assesses defect type, shunt direction, RV size, pulmonary pressures, and associated lesions.
- TOE / transoesophageal echo: useful for detailed anatomy and planning device closure in suitable cases.
- Cardiac MRI: helpful when anatomy is complex, especially in sinus venosus defects or if pulmonary venous drainage needs clarification.
- Right heart catheterisation: may be used when pulmonary vascular resistance, shunt magnitude, or operability needs clarification.
⚠️ Complications
- 💨 Pulmonary hypertension
- 📉 Right heart enlargement and eventual right heart failure
- ❤️ Atrial arrhythmias such as atrial flutter or AF, especially in adulthood
- 🧠 Paradoxical embolism causing stroke or systemic embolism
- 🔄 Eisenmenger syndrome in late untreated severe disease
💊 Management
- Monitoring: small, haemodynamically insignificant ASDs may be followed with periodic echocardiography.
- Closure is usually indicated when:
- there is a haemodynamically significant left-to-right shunt, and
- there is right-heart enlargement, with or without symptoms.
- Qp:Qs: a ratio >1.5:1 is often used as a supporting threshold for a significant shunt.
- Catheter device closure: suitable for many secundum ASDs when anatomy is favourable.
- Surgical closure: usually needed for primum defects, sinus venosus defects, and some large or anatomically unsuitable secundum ASDs.
- Do not close the defect in advanced irreversible pulmonary vascular disease / Eisenmenger physiology, because this can worsen right-sided failure.
- Arrhythmia / embolic management: anticoagulation may be needed for AF according to AF guidance; paradoxical embolism should prompt specialist review and closure assessment.
- Prognosis: generally excellent when significant defects are repaired before major pulmonary vascular disease develops.
🦷 Infective Endocarditis Advice
- 💉 Routine antibiotic prophylaxis is not recommended for dental procedures under NICE guidance.
- 🪥 Good oral hygiene and regular dental care remain important.
- 🩺 After repair, endocarditis prophylaxis is generally only relevant for a limited period or if there is a residual defect adjacent to prosthetic material, according to specialist guidance.
📌 High-yield exam pearl: In ASD, the murmur comes from increased pulmonary flow, not turbulent flow through the defect. 🔊 A fixed split S2 in an otherwise well child or young adult is a classic clue. ⚠️ Think of closure when there is RV dilatation, even if the patient feels well.
🩺 Case 1 - Child with Recurrent Chest Infections
A 6-year-old girl is evaluated for recurrent chest infections and poor growth. Examination reveals a fixed split second heart sound and a systolic murmur at the left upper sternal edge. Echocardiography shows a secundum ASD with right atrial and right ventricular dilatation. Management: 🩺 Elective closure is appropriate because the defect is haemodynamically significant and the right heart is enlarged. If anatomy is suitable, this may be by percutaneous device closure; otherwise surgical repair is used. Avoid: ❌ Delaying closure once a significant shunt with right-heart volume overload is established.
🩺 Case 2 - Adult with Incidental Murmur
A 35-year-old woman is found to have a murmur during a routine check. She is asymptomatic, but echo demonstrates a secundum ASD with Qp:Qs >1.5:1 and RV dilatation. Management: 💊 Closure is generally indicated because the shunt is significant and causing right-heart enlargement, even though she has no symptoms. Avoid: ❌ Assuming “asymptomatic” means harmless - untreated ASD can still lead to atrial arrhythmias, RV failure, and pulmonary vascular disease over time.
🩺 Case 3 - Older Patient with Pulmonary Hypertension
A 70-year-old man presents with exertional dyspnoea and ankle swelling. Examination shows elevated JVP, a loud P2, and signs of right heart failure. Echo confirms an unrepaired ASD with severe pulmonary hypertension. Management: 🚑 Refer to specialist congenital / pulmonary hypertension services. Give supportive treatment for right heart failure. If pulmonary vascular disease is advanced and the shunt has become right-to-left or bidirectional, closure is not advised. Avoid: ❌ Closing the defect in irreversible pulmonary vascular disease, as this can worsen haemodynamics and right-sided failure.
📚 References
- 🌍 ESC Guidelines for Adult Congenital Heart Disease.
- 📘 NICE CG64: Prophylaxis against infective endocarditis.
- 🏥 MSD / Merck Manual Professional: Atrial Septal Defect (ASD).
- 🫀 Specialist congenital cardiology guidance on ASD assessment and closure.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery