Related Subjects: Small Bowel Obstruction
|Colonic (Large bowel) Obstruction
|Caecal Volvulus
|Small Bowel Ischemia
|Hartmann's procedure
|Sigmoid Volvulus
|Acute Colonic Pseudo-obstruction
| Metabolic acidosis
| Lactic acidosis
|Rectal Prolapse
|Anal Cancer
|Anal Fissure
|Pilonidal Abscess (sinus)
|Haemorrhoids (Piles)
|Hartmann's procedure
🚨 Mesenteric Ischaemia carries a mortality of up to 80%, even when diagnosis and treatment are prompt.
Delay in recognition is the biggest killer - pain out of proportion to examination is the key clinical clue. ⚠️
📖 About
- Presentation can be acute (sudden embolus) or chronic (“abdominal angina”).
- Symptoms often outweigh signs until late → peritonitis appears once infarction occurs.
- Pathology may involve arterial thrombosis, embolism, venous thrombosis, or non-occlusive ischaemia (e.g. low flow states, vasopressors).
🩻 Anatomy
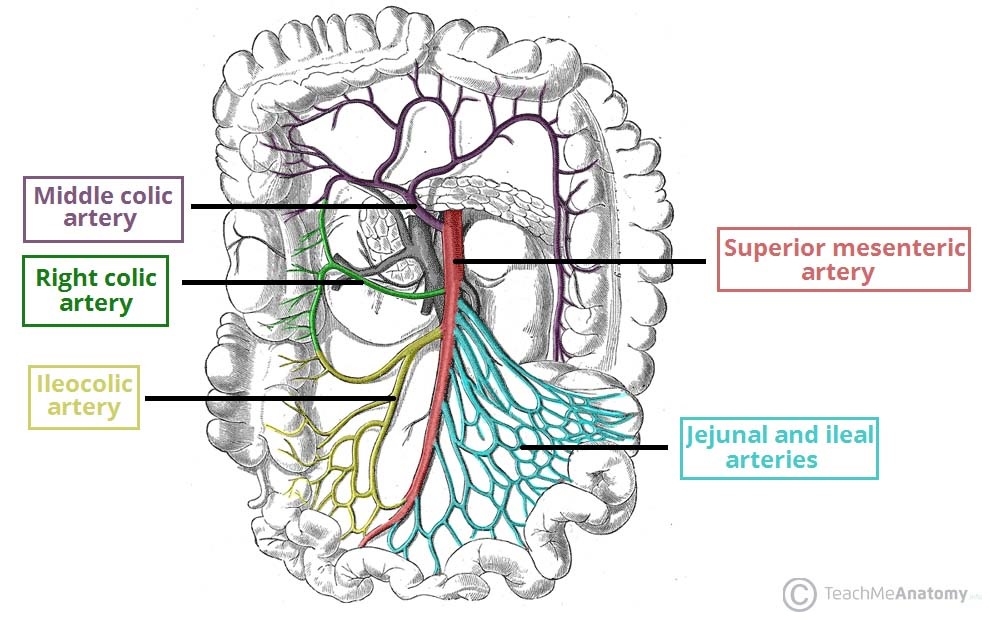
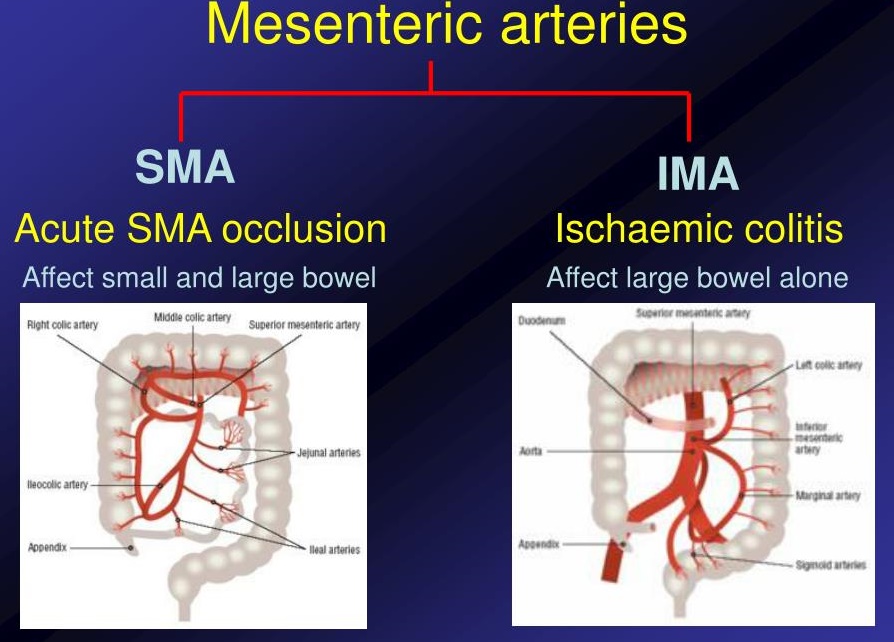
- Superior mesenteric artery (SMA) supplies midgut (duodenum → proximal 2/3 transverse colon).
- Collateral supply may temporarily mask symptoms until demand exceeds flow.
🧬 Aetiology
- Atherosclerotic thrombosis 🧱: Most common in chronic disease; often SMA origin.
- Embolism 🫀: Classically from atrial fibrillation, mural thrombus post-MI, prosthetic valves.
- Thrombophilia 🩸: Hypercoagulable states (polycythaemia, dehydration, malignancy).
- Venous occlusion: Mesenteric venous thrombosis (rare, associated with cirrhosis, OCP use, portal HTN).
- Non-occlusive ischaemia: Critically ill, shock, vasopressor therapy → gut hypoperfusion.
- Untreated → transmural necrosis ➡️ perforation ➡️ peritonitis.
👩⚕️ Clinical Presentation
- Acute: Sudden, severe abdominal pain out of proportion to clinical findings.
- Chronic: Post-prandial pain (intestinal angina) → fear of eating → weight loss.
- Diarrhoea (may be bloody), nausea, vomiting.
- Late: Peritonitis, sepsis, shock.
🧪 Investigations
- Bloods: Elevated WCC, CRP, renal impairment (prerenal AKI), metabolic acidosis.
- ABG: Raised lactate = ischaemia/necrosis ⚠️.
- AXR: Non-specific; may show dilated loops or “thumb-printing”.
- ECG: Check for AF/MI; troponin if suspicion.
- CT Angiography (CTA) 📊: Investigation of choice → detects vessel occlusion, pneumatosis, portal venous gas.
- Catheter Angiography: Gold standard, also therapeutic (thrombectomy, vasodilators).
💊 Management
- Immediate resuscitation: Oxygen, IV fluids, broad-spectrum antibiotics, NG decompression.
- Anticoagulation: IV heparin if embolic/thrombotic origin suspected.
- Emergency Surgery 🪡: Laparotomy + resection of necrotic bowel; sometimes “second look” laparotomy at 24–48 hrs.
- Endovascular: Angioplasty, embolectomy, or intra-arterial vasodilators for non-occlusive ischaemia.
- Palliative care: In frail patients with extensive infarction and poor prognosis.
⚖️ Prognosis & Key Teaching Points
- Mortality is high due to diagnostic delay → think early in elderly with AF + abdominal pain.
- Pain out of proportion to signs = classic exam and clinical red flag 🚨.
- CTA has replaced plain AXR as the main diagnostic test.
- Early anticoagulation and surgery save lives; late presentation often fatal.
📚 References
