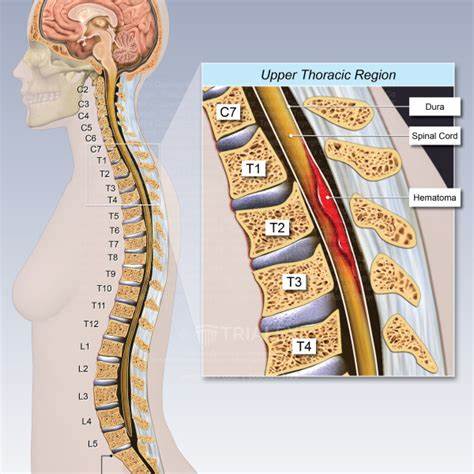
Spinal Cord Haematoma
Related Subjects:
|Transverse myelitis
|Acute Disseminated Encephalomyelitis
|Cervical spondylosis
|Spinal Cord Anatomy
|Acute Disc Prolapse
|Spinal Cord Compression
|Spinal Cord Haematoma
|Foix-Alajouanine syndrome
|Cauda Equina
|Conus Medullaris syndrome
|Anterior Spinal Cord syndrome
|Central Spinal Cord syndrome
|Brown-Sequard Spinal Cord syndrome
|Internal Decapitation
🚨 Neurological & Neurosurgical Emergency - spinal cord haematoma requires urgent recognition and action. Delay in diagnosis can result in permanent paralysis or death.
📖 About
- Spinal Cord Haematoma: 🩸 Rare but potentially life-threatening condition where bleeding occurs in or around the spinal cord.
- Can be epidural (outside dura, compresses cord), subdural, or intramedullary (within cord tissue).
- Classically presents with sudden, excruciating spinal pain → followed rapidly by acute myelopathy (weakness, sensory loss, sphincter disturbance).
🧬 Causes
- Vascular malformations: AVMs, cavernomas, angiomas.
- Anticoagulation / coagulopathy: Warfarin, heparin, DOACs, haemophilia, thrombocytopenia.
- Iatrogenic: Following lumbar puncture or spinal anaesthesia.
- Spinal cord trauma or surgery.
- Spinal tumours or syringomyelia (predisposing to fragile vessels).
- Rarely: inflammatory causes like transverse myelitis with associated bleeding.
🩺 Clinical Presentation
- ⚡ Sudden, severe back or neck pain, often described as “tearing” or “knife-like.”
- Weakness - initially flaccid (LMN) → may evolve to spastic (UMN).
- 🔻 Sensory level below lesion (loss of pain, temperature, ± dorsal column sparing).
- 🚽 Bowel and bladder dysfunction early in course.
- Symptoms can mimic acute transverse myelitis or cord infarction - but the hyperacute onset is a clue.
🔍 Investigations
- MRI with/without gadolinium: Gold standard - defines site, extent, and differentiates haematoma from tumour or abscess.
- CT spine: May detect blood if MRI unavailable, but less sensitive for intramedullary lesions.
- Bloods: INR, platelets, coagulation profile - assess anticoagulation status.
💊 Management
- 🚨 Immediate reversal of anticoagulation: Vitamin K + Prothrombin Complex Concentrate (PCC, e.g., Octaplex/Beriplex) for warfarin; protamine for heparin.
- 🔪 Surgical clot evacuation (laminectomy or microsurgical decompression): Indicated if significant or progressive neurological deficit.
- Conservative management: Rare; only considered in small haematomas with mild, stable symptoms and no progression.
- Treat underlying cause (e.g., resection of AVM, correct bleeding disorder).
- Spinal neurorehabilitation: Physiotherapy, occupational therapy, bladder/bowel programmes, psychological support.
