Related Subjects:
|Metabolic acidosis
|Lactic acidosis
|Acute Kidney Injury (AKI) / Acute Renal Failure
|AP of the Kidneys
|Chronic Kidney Disease (CKD)
|Anaemia in Chronic Kidney Disease
|Analgesic Nephropathy
|Medullary Sponge kidney
|IgA Nephropathy (Berger's disease)
|HIV associated nephropathy (HIVAN)
The kidneys are paired, retroperitoneal organs (approximately T12–L3; left often slightly higher) that maintain homeostasis by regulating extracellular volume, electrolytes, acid–base balance, and blood pressure, while excreting metabolic waste and drugs. They receive a disproportionately high blood flow (~20–25% of cardiac output), making them excellent “filters” but also vulnerable to hypoperfusion and nephrotoxins (important in AKI pathways).
🩻 Gross Anatomy
- Location: Retroperitoneal, either side of spine; protected by lower ribs and posterior abdominal wall muscles.
- Coverings: Fibrous capsule → perinephric fat → renal fascia (Gerota’s) → paranephric fat.
- Hilum: Medial indentation where renal vein, renal artery, lymphatics, nerves, and renal pelvis/ureter pass.
- Remember: Vein (anterior) → Artery → Pelvis/ureter (posterior) (V-A-P).
- Cortex: Glomeruli + proximal & distal tubules; high blood flow; highly metabolic.
- Medulla: Pyramids containing loops of Henle and collecting ducts; relatively low oxygen tension → prone to hypoxic injury.
- Papilla: Tip of pyramid draining into minor calyx → major calyx → renal pelvis → ureter.
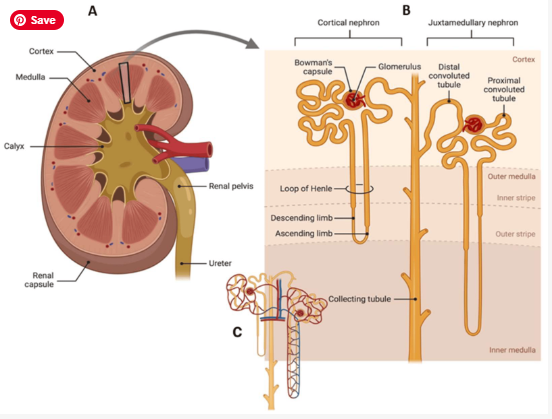
🧬 Microanatomy: The Nephron (Functional Unit)
Each kidney contains ~1–1.5 million nephrons. Renal function is the sum of filtration at the glomerulus plus selective tubular reabsorption and secretion. Nephrons are broadly cortical (most; short loops) and juxtamedullary (fewer; long loops essential for urine concentration).
| Segment 🧩 |
Key transport & physiology ⚙️ |
High-yield clinical links 🩺 |
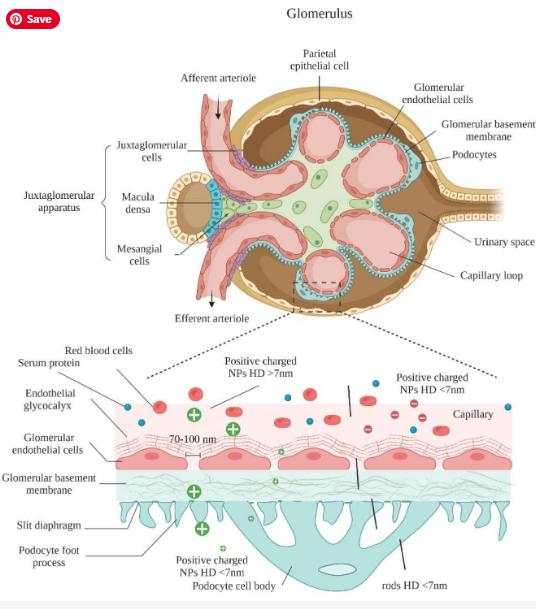
| Glomerulus + Bowman’s capsule (renal corpuscle) |
- Ultrafiltration driven by Starling forces (capillary hydrostatic pressure minus opposing forces).
- Filtration barrier: fenestrated endothelium + GBM (negatively charged) + podocyte slit diaphragm.
- Selective: water/small solutes filter; cells & most proteins retained.
|
- Proteinuria suggests barrier injury (podocytopathy/GBM disease).
- Haematuria + proteinuria → think glomerulonephritis.
- Changes in afferent/efferent tone alter GFR (e.g., NSAIDs vs ACEi/ARB).
|
| Proximal tubule (PCT) 🧽 |
- Bulk reabsorption: ~65–70% filtered Na⁺/water; most HCO₃⁻; ~100% glucose & amino acids (until transporters saturate).
- Na⁺ reabsorption powers most solute uptake (Na⁺/H⁺ exchanger, cotransporters).
- Secretes organic anions/cations (many drugs), creatinine, urate (bidirectional handling).
|
- SGLT2 inhibitors act here → glycosuria/diuresis.
- Fanconi syndrome: PCT dysfunction → glycosuria (with normal glucose), phosphaturia, aminoaciduria, proximal RTA.
- Many nephrotoxins injure PCT (high metabolic demand).
|
| Loop of Henle 🔁 |
- Descending limb: water-permeable → water exits into hypertonic medulla.
- Thick ascending limb (TAL): water-impermeable; reabsorbs Na⁺/K⁺/2Cl⁻ (NKCC2) → “diluting segment”.
- Creates medullary gradient via countercurrent multiplication.
|
- Loop diuretics (furosemide) inhibit NKCC2 → powerful natriuresis; can cause hypokalaemia, metabolic alkalosis.
- Medulla has low O₂ → susceptible to hypoxic injury; concentrating defects may appear early.
|
| Distal convoluted tubule (DCT) 🎛️ |
- Reabsorbs NaCl via NCC (thiazide-sensitive); relatively water-impermeable.
- Key site for Ca²⁺ reabsorption (PTH-regulated).
|
- Thiazides inhibit NCC → can raise serum Ca²⁺ (useful in calcium stone formers).
- Electrolyte disturbances: hyponatraemia, hypokalaemia.
|
| Collecting duct 🚰 |
- Principal cells: Na⁺ reabsorption (ENaC) and K⁺ secretion; aldosterone ↑ ENaC/Na⁺-K⁺ ATPase.
- Intercalated cells: acid–base balance (H⁺ secretion / HCO₃⁻ handling).
- ADH inserts aquaporin-2 in collecting duct → water reabsorption and concentrated urine.
|
- Diabetes insipidus: impaired ADH effect → polyuria/polydipsia, dilute urine.
- Hyperkalaemia worsened by hypoaldosteronism/RAAS blockade; improved by mineralocorticoids (selected cases).
- Type 1/2 RTA patterns relate to collecting duct function.
|
🫀 Renal Blood Supply & Microcirculation
Renal perfusion is high to support filtration, but intrarenal oxygenation is uneven: the cortex is well perfused, while the medulla operates at low oxygen tension. This is why hypoperfusion, sepsis, and vasoconstrictors can precipitate AKI, and why the medulla is particularly vulnerable.
- Arterial tree: Renal artery → segmental → interlobar → arcuate → interlobular (cortical radial) → afferent arterioles.
- Afferent arteriole → glomerulus → efferent arteriole (unique “two arterioles in series” arrangement).
- Efferent arteriole branches:
- Peritubular capillaries (cortex): support reabsorption/secretion.
- Vasa recta (medulla): countercurrent exchange preserves medullary gradient.
🧠 Renal Innervation & Hormonal Control
- Sympathetic (dominant): vasoconstriction (↓ renal blood flow), ↑ renin release, ↑ tubular Na⁺ reabsorption (stress/volume depletion response).
- RAAS: renin → angiotensin II (efferent constriction, ↑ proximal Na⁺ reabsorption) → aldosterone (ENaC ↑, K⁺ excretion ↑).
- Natriuretic peptides (ANP/BNP): promote natriuresis (↑ GFR, ↓ Na⁺ reabsorption) in volume overload states.
- ADH (vasopressin): water retention via aquaporin-2 insertion in collecting duct.
🧪 Core Physiology Themes (High-Yield)
| Theme 📌 |
What’s happening? 🧠 |
Clinical relevance 🩺 |
| Glomerular filtration (GFR) |
Filtration depends on renal plasma flow and the balance of forces across the glomerular capillary. Afferent tone controls inflow; efferent tone controls outflow pressure and filtration fraction.
|
NSAIDs (afferent constriction) and ACEi/ARB (efferent dilation) can reduce GFR-especially in hypovolaemia, CKD, or renal artery stenosis.
|
| Autoregulation 🎚️ |
Kidneys stabilise GFR across a BP range using the myogenic response and tubuloglomerular feedback (macula densa sensing distal NaCl).
|
In shock/sepsis, autoregulation can fail → AKI risk rises. Careful fluid/blood pressure strategy matters.
|
| Countercurrent system 🔁 |
Juxtamedullary loops generate a corticomedullary osmotic gradient (multiplication) while vasa recta preserve it (exchange). ADH then “uses” this gradient to reclaim water in collecting ducts.
|
Early tubular injury often presents as impaired concentrating ability (polyuria, low urine osmolality) before creatinine rises.
|
| Acid–base handling ⚗️ |
PCT reabsorbs most filtered bicarbonate; distal nephron generates “new” bicarbonate and excretes acid (as NH₄⁺ and titratable acids). Intercalated cells are key.
|
Renal tubular acidosis patterns map to segment dysfunction (proximal vs distal) and have characteristic electrolyte profiles.
|
📊 Cortex vs Medulla - Quick Comparison
| Feature |
Cortex |
Medulla |
| Main structures |
Glomeruli, PCT, DCT |
Loops of Henle, collecting ducts, vasa recta |
| Perfusion |
High (majority of renal blood flow) |
Low (physiologically low O₂) |
| Key job |
Filtration + bulk reabsorption/secretion |
Urine concentration (osmotic gradient) |
| Vulnerability |
Perfusion-dependent; AKI in shock |
Hypoxia prone; concentrating defects early |
🧠 Clinical Pearls (Renal Physiology → Bedside)
- 🩸 High flow, uneven oxygenation: cortex is well perfused; medulla is “on the edge” → hypoperfusion can cause tubular injury disproportionately.
- 💊 Drug effects map to anatomy: loop diuretics (TAL), thiazides (DCT), ACEi/ARB (efferent tone/RAAS), NSAIDs (afferent tone/prostaglandins).
- 🚑 Concentrating ability can fail early: tubular dysfunction may precede creatinine rise (watch urine output and osmolality when available).
- 🧪 Proteinuria is a glomerular clue: suggests filtration barrier injury-especially if persistent or heavy.
📝 Summary
Renal structure is tightly linked to renal function: glomeruli filter, PCT bulk-reabsorbs, the loop of Henle builds the medullary gradient, DCT fine-tunes electrolytes, and the collecting duct performs final water and acid–base control under ADH and aldosterone. The kidney’s unique “afferent → glomerulus → efferent” microcirculation supports filtration but creates segment-specific vulnerabilities-particularly medullary hypoxia and tubular injury in AKI.
