Sideroblastic Anaemia
Related Subjects:
| Sideroblastic Anaemia
| Splenectomy
📘 About
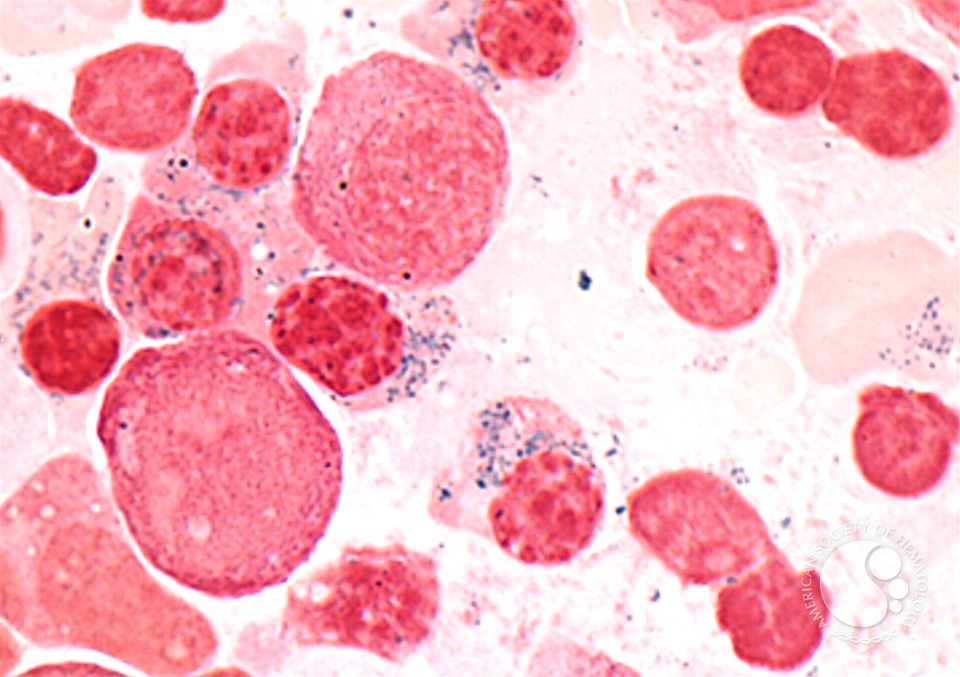
- Sideroblastic anaemia is a rare form of anaemia characterised by ineffective erythropoiesis and the presence of ring sideroblasts in the bone marrow.
- Sideroblasts are erythroblasts (immature RBCs) with iron-loaded mitochondria encircling the nucleus (seen with Prussian Blue stain).
- Iron is available but cannot be incorporated into haem → leading to anaemia + systemic iron overload.
⚙️ Pathophysiology / Aetiology
- Final step in haem synthesis (ferrochelatase inserts Fe2+ into protoporphyrin IX) is impaired.
- Alcohol: interferes with pyridoxal-5’-phosphate (B6), a cofactor for ALAS (aminolevulinic acid synthase).
- Lead: inhibits ferrochelatase and ALA dehydratase.
- Hereditary forms: ALAS2 mutation (X-linked), ferrochelatase deficiency.
- Iron overload results from ineffective erythropoiesis, sometimes leading to hepatosplenomegaly.
🩺 Clinical Presentation
- Fatigue, weakness, pallor.
- Flow murmurs (high-output state due to anaemia).
- Hepatosplenomegaly from iron deposition.
- History: alcohol, drugs (isoniazid, pyrazinamide), family history.
🧪 Causes of Sideroblastic Anaemia
| Cause | Mechanism | Examples |
|---|
| Acquired – Toxins | Disrupt haem synthesis | Alcohol, Lead |
| Acquired – Drugs | Block B6 metabolism | Isoniazid, Pyrazinamide |
| Myelodysplastic syndromes (MDS) | Ineffective erythropoiesis | Refractory anaemia with ring sideroblasts (RARS) |
| Hereditary | Genetic enzyme defects | ALAS2 mutation, ferrochelatase deficiency |
🔎 Investigations
- Blood film: dimorphic picture (mix of microcytic & normocytic cells).
- Hypochromic microcytic anaemia common.
- Bone marrow biopsy: ring sideroblasts with perinuclear iron granules (Prussian Blue).
- Iron studies: ↑ serum iron, ↑ ferritin, ↑ transferrin saturation.
- Consider LFTs and genetic testing if hereditary suspected.
⚕️ Management
- Address underlying cause: stop alcohol, remove toxins/drugs.
- Pyridoxine (B6) trial: particularly in hereditary/ALAS2-related cases.
- Supportive: blood transfusions (but ↑ iron overload risk).
- Iron overload: consider iron chelation (e.g., deferoxamine).
- In severe/refractory cases: erythropoietin (EPO) or haematopoietic stem cell transplantation.
📚 References
- BNF – Anaemia management
- NICE CKS – Anaemia (non-iron deficiency)
- Hoffbrand’s Essential Haematology
Cases - Sideroblastic Anaemia
- Case 1 - Congenital form 👶: A 4-year-old boy is investigated for pallor and lethargy. Bloods: microcytic anaemia (Hb 8.5 g/dL, MCV 65 fL), high ferritin, high serum iron. Bone marrow: ring sideroblasts on Prussian blue staining. Family history: X-linked disorder. Diagnosis: congenital sideroblastic anaemia. Managed with pyridoxine supplementation and transfusion support.
- Case 2 - Acquired secondary (alcohol/toxin) 🍺: A 52-year-old man with chronic alcohol misuse presents with fatigue and breathlessness. Bloods: microcytic, hypochromic anaemia with raised serum iron. Bone marrow aspirate: ring sideroblasts. Diagnosis: acquired sideroblastic anaemia secondary to alcohol. Managed with alcohol cessation, pyridoxine, and supportive care.
- Case 3 - Myelodysplastic syndrome (clonal) 🧬: A 68-year-old woman presents with progressive anaemia and easy bruising. Bloods: Hb 9.0 g/dL, macrocytic indices, raised ferritin. Bone marrow: dysplastic changes with ring sideroblasts. Diagnosis: sideroblastic anaemia associated with MDS (RARS subtype). Managed with transfusions, iron chelation, and consideration of disease-modifying therapy (lenalidomide, azacitidine).
Teaching Point 🩺: Sideroblastic anaemia is characterised by defective haem synthesis → iron trapped in mitochondria around erythroblast nuclei (ring sideroblasts). Causes: congenital (X-linked), acquired (alcohol, lead, drugs, B6 deficiency), clonal (MDS). Iron studies: ↑ ferritin, ↑ serum iron, normal/↑ transferrin saturation. Management is cause-specific (e.g. pyridoxine, toxin removal, MDS therapy).
