
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Diabetes Mellitus Type 1 and DKA (children)
Related Subjects:Sick Neonate |APGAR Scoring |Approach to Assessing Sick Child |Sick Child with Acute Gastroenteritis |Sick Child with Respiratory Distress |Sick child Diabetes Mellitus Type 1 and DKA
💉 Type 1 Diabetes Mellitus (T1DM) is a chronic autoimmune condition caused by destruction of pancreatic β-cells ➝ absolute insulin deficiency ➝ persistent hyperglycaemia. Around 25% of children present in Diabetic Ketoacidosis (DKA) at first diagnosis 🚨.
📖 About
- Autoimmune destruction of insulin-producing β-cells in the pancreas.
- Usually presents in childhood or adolescence, though can occur at any age.
- Requires lifelong insulin therapy.
🧬 Aetiology
- Insulin produced by islets of Langerhans (β-cells).
- Autoantibodies (e.g. anti-GAD, anti-islet cell) target β-cells, leading to progressive destruction.
- Genetic predisposition (HLA types), with environmental triggers (viral infections, toxins) thought to play a role.
🩺 Clinical Features
- Classic triad: Polyuria 🚽, Polydipsia 💧, Weight loss ⚖️.
- Vomiting, lethargy, and dehydration in severe cases.
- Nocturnal enuresis (bedwetting) may be a presenting sign.
- Recurrent candida infections can be a clue.
- 25% present in DKA (abdominal pain, vomiting, Kussmaul breathing, acetone breath).
🧪 Investigations
- Blood glucose: Random ≥11.1 mmol/L with symptoms is diagnostic.
- Ketones: Urine or blood ketones (raised in DKA).
- HbA1c: Chronic hyperglycaemia marker (≥48 mmol/mol).
- Blood gas: Metabolic acidosis in DKA (pH <7.3, HCO₃⁻ <15).
- Autoantibodies: Anti-GAD, anti-islet cell (autoimmune confirmation).
- Screen for coeliac and thyroid disease (autoimmune associations).
💊 General Management of T1DM
- Education 👨👩👧: Self-monitoring of glucose, insulin administration, sick-day rules.
- Insulin therapy:
- Basal-bolus: Long-acting insulin once daily + rapid insulin with meals.
- Pump therapy: Subcutaneous infusion in selected children; risks: infection, pump failure.
- Diet & lifestyle: Carbohydrate counting, healthy diet, regular exercise.
🚨 Paediatric Diabetic Ketoacidosis (DKA) Management
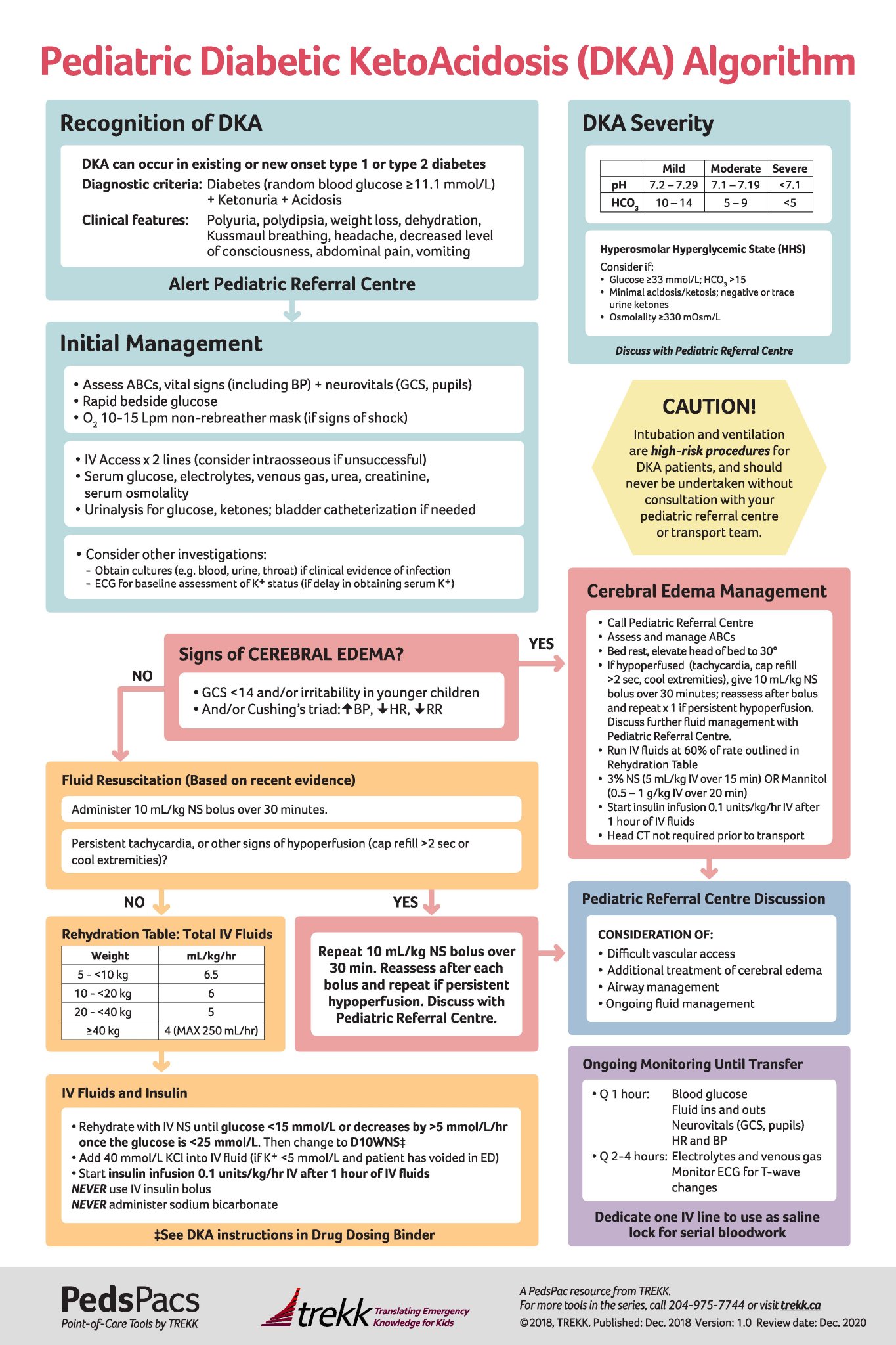
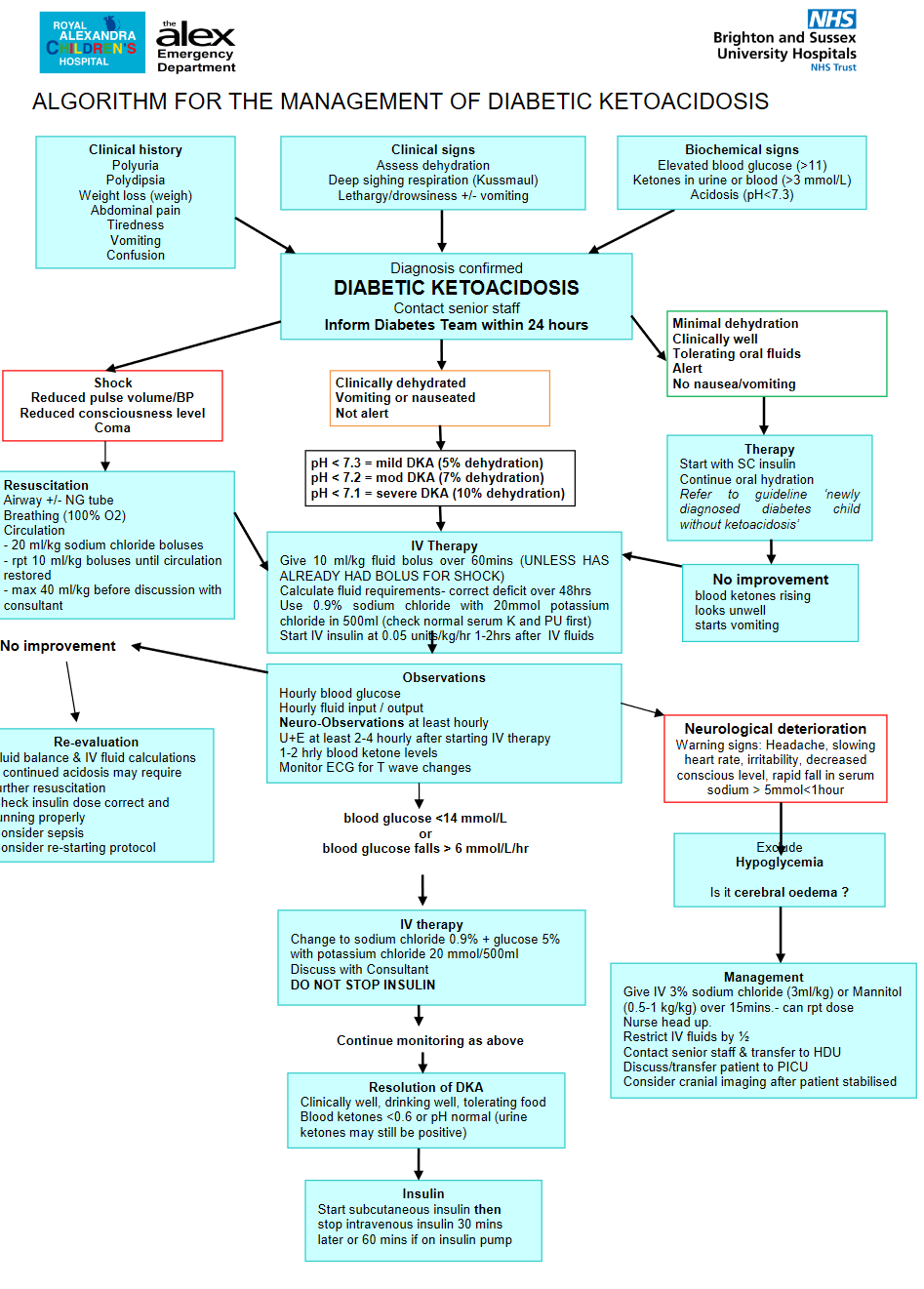
⚠️ Cerebral oedema is the most feared complication in paediatric DKA. Always monitor neurological status closely. Treat promptly with mannitol 20% (2.5 mL/kg IV over 10 min) or 3% hypertonic saline (5 mL/kg IV over 10–15 min) if suspected.
🩺 Stepwise Management
- 1️⃣ ABC & Monitoring
- Airway, Breathing, Circulation ➝ stabilise.
- Continuous monitoring: HR, BP, SpO₂, GCS, neuro obs hourly.
- Cardiac monitor (risk of arrhythmia if K⁺ deranged).
- 2️⃣ IV Access & Bloods
- Venous gas (pH, bicarbonate, ketones).
- FBC, U&E, glucose, lactate.
- Urinalysis for ketones.
- 3️⃣ Fluids 💧
- Correct dehydration slowly over 48 h (avoid cerebral oedema).
- Use 0.9% saline ± 5% dextrose when BG <14 mmol/L.
- Resus if shocked: 10 mL/kg 0.9% saline over 10–15 min (repeat once if needed).
- 4️⃣ Insulin 💉
- Start 1–2 h after fluids have begun.
- Continuous IV infusion at 0.05–0.1 units/kg/hr.
- Aim: fall in glucose 2–5 mmol/L/hr.
- 5️⃣ Potassium ⚡
- Total body K⁺ depleted even if serum appears normal/high.
- Add KCl once child is voiding and serum K⁺ <6 mmol/L.
- Typical: 20 mmol KCl per 500 mL bag.
- 6️⃣ Ongoing Care
- Hourly BG; 2–4 hourly VBG & electrolytes.
- Strict fluid balance (catheterise if necessary).
- Watch for headache, bradycardia, ↓GCS ➝ suspect cerebral oedema.
- 7️⃣ Transition to SC Insulin
- When ketones cleared, child well, eating & drinking.
- Overlap IV infusion with first SC dose by 30–60 min.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery