Bleeding Antepartum
⚠️ Antepartum haemorrhage (APH) = vaginal bleeding after 24 weeks until delivery.
Occurs in ~3–5% of pregnancies and is a major cause of maternal & perinatal morbidity/mortality.
💡 Uterine blood flow at term is 600–800 mL/min → even short delays can be catastrophic.
📊 Incidence
- 3–5% of pregnancies.
- Still one of the leading causes of maternal and fetal death worldwide.
🔎 Causes of APH
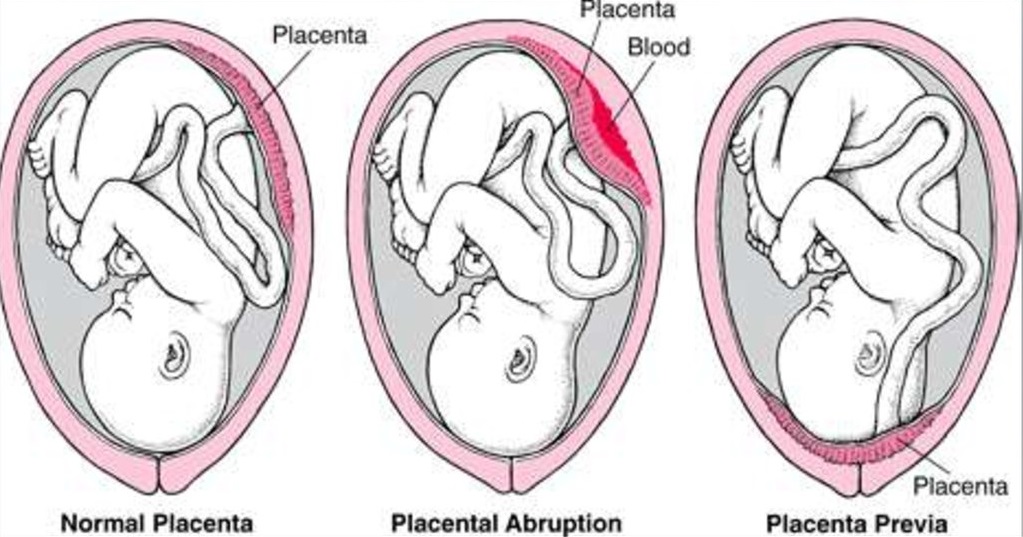
- 🌸 Placenta praevia (~1:200 pregnancies)
– Painless bright red bleeding.
– Placenta partially/completely covers os.
– Diagnosed by TVS (transvaginal safest).
– ⚠️ Never do PV exam before praevia excluded.
- 💥 Placental abruption
– Premature detachment of placenta.
– Painful, tense (“woody”) uterus, bleeding (revealed or concealed).
– RFs: pre-eclampsia, smoking, cocaine, trauma.
– Complications: DIC, fetal compromise, renal failure.
- 🚨 Vasa praevia (~1:2500)
– Fetal vessels cross near os → rupture after ROM.
– Presents with PV bleed + fetal HR decelerations.
– Dx: USS with Doppler.
– ⚡ Emergency C-section needed.
- 🧩 Other: circumvallate placenta, cervicitis, cervical polyps, malignancy.
- ❓ Unexplained: ~50% have no identifiable cause but still ↑ perinatal risk.
🩺 Clinical Features
- Praevia: painless, soft uterus, normal FHR.
- Abruption: painful, tense uterus, abnormal FHR.
- Vasa praevia: bleeding + fetal HR changes after ROM.
- Maternal obs, fetal movements, CTG essential.
- ⚠️ Avoid PV exam until praevia excluded on scan.
📏 Severity of Bleed
- Spotting → minor (<50 mL, settled).
- Major → 500–1000 mL, stable.
- Massive → >1000 mL ± maternal shock.
🧪 Investigations
- 🩸 Bloods: FBC, group & save / X-match ≥4 units, clotting, U&E, LFTs.
- 💉 Kleihauer test if Rh− → guides anti-D.
- 🧪 Urinalysis: check proteinuria (pre-eclampsia).
- 📊 CTG: assess fetal wellbeing.
- 🧲 USS: TVS for placental localisation, Doppler for vasa praevia.
🏥 Management
- 🚑 Resuscitation (ABC): O₂, 2x wide-bore IVs, fluids, blood products (O-neg if urgent).
- 📞 Call senior help: obstetrician, anaesthetist, neonatology team.
- 💊 Steroids: 24–34+6 wks if preterm delivery likely.
- 🚺 Placenta praevia: elective C-section if placenta <2 cm from os.
- 💥 Abruption: manage shock (concealed bleed often > visible loss), correct DIC, expedite delivery if unstable.
- ⚡ Massive haemorrhage: Activate major obstetric haemorrhage protocol → immediate delivery (often C-section).
- ➕ Don’t forget: anti-D for Rh−, catheter for fluid balance, monitor urine output.
⚠️ Maternal Complications
- Anaemia, hypovolaemic shock.
- DIC, renal failure (ATN).
- PPH (~25% after abruption).
- Infection, Sheehan’s syndrome, transfusion risks.
⚠️ Fetal Complications
- Hypoxia, IUFD.
- Prematurity, growth restriction.
📌 Exam Pearls
- Praevia = painless + normal FHR.
- Abruption = painful + abnormal FHR.
- Vasa praevia = bleed + FHR drop post-ROM.
- Shock may be concealed → treat aggressively.
- Always ask: maternal stability? fetal compromise? → delivery timing depends on both.
📖 References
