
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
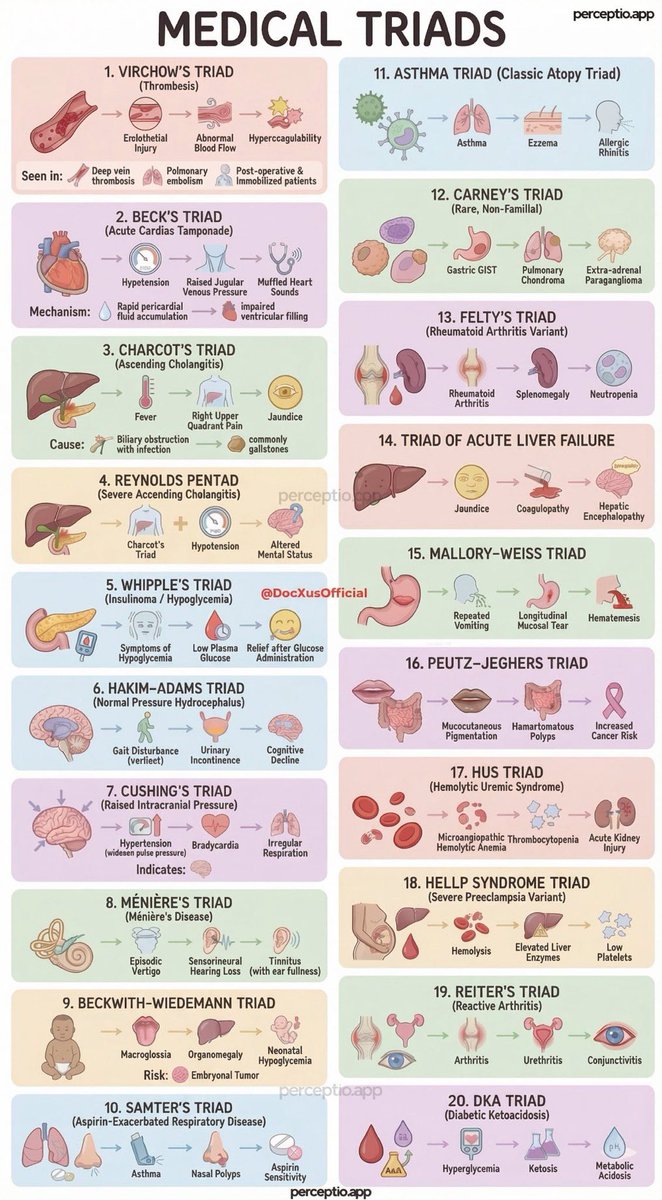
Famous Medical Triads
| Triad Name | Components | Condition / Context | Teaching & Pathophysiology Pearl |
|---|---|---|---|
| Charcot’s Triad | RUQ pain
Fever Jaundice |
Ascending cholangitis | Reflects biliary obstruction + infection → add hypotension & confusion = Reynolds’ pentad (sepsis). |
| Virchow’s Triad | Stasis
Endothelial injury Hypercoagulability |
Venous thromboembolism | Explains peri-operative, malignancy and immobility risk. |
| Beck’s Triad | Hypotension
Raised JVP Muffled heart sounds |
Cardiac tamponade | Obstructive shock physiology → impaired ventricular filling. |
| Cushing’s Triad | Hypertension
Bradycardia Irregular respirations |
Raised intracranial pressure | Late sign of impending brain herniation. |
| Whipple’s Triad | Hypoglycaemic symptoms
Low plasma glucose Relief with glucose |
True hypoglycaemia | Confirms symptoms are causally linked to hypoglycaemia. |
| Wernicke’s Triad | Confusion
Ataxia Ophthalmoplegia |
Wernicke encephalopathy | Thiamine deficiency - triad often incomplete; treat before glucose. |
| HUS Triad | AKI
MAHA Thrombocytopenia |
Haemolytic uraemic syndrome | Microangiopathy → avoid antibiotics in acute E. coli O157. |
| HELLP Triad | Haemolysis
Elevated LFTs Low platelets |
Severe pre-eclampsia variant | Placental endothelial dysfunction → definitive treatment is delivery. |
| Horner’s Triad | Ptosis
Miosis Anhidrosis |
Sympathetic chain lesion | Think carotid dissection, Pancoast tumour, brainstem stroke. |
| Saint’s Triad | Hiatus hernia
Gallstones Diverticular disease |
Degenerative GI association | Association only - not causative. |
| Murphy’s Surgical Triad | RUQ pain
Fever Leukocytosis |
Acute cholecystitis | Inflammatory obstruction of cystic duct. |
| Appendicitis Triad | Migratory pain
Anorexia Low-grade fever |
Acute appendicitis | Visceral → parietal peritoneal irritation explains pain shift. |
| Boerhaave’s Triad | Vomiting
Chest pain Surgical emphysema |
Oesophageal rupture | Transmural tear → mediastinitis (high mortality). |
| Bowel Obstruction Triad | Colicky pain
Vomiting Distension |
Mechanical obstruction | Constipation is common but not universal. |
| Trauma Triad of Death | Hypothermia
Acidosis Coagulopathy |
Major trauma | Self-perpetuating lethal cycle - correct early. |
| Concussion Triad | LOC
Amnesia Headache |
Mild traumatic brain injury | Normal CT does not exclude significant injury. |
| Epidural Haematoma Triad | Lucid interval
Rapid deterioration Fixed dilated pupil |
MMA bleed | Arterial bleed → time-critical neurosurgery. |
| Flail Chest Triad | Paradoxical movement
Respiratory distress Chest wall pain |
Blunt thoracic trauma | Often compounded by pulmonary contusion. |
| Pelvic Fracture Triad | Pelvic pain
Shock Perineal bruising |
High-energy trauma | Pelvis can conceal massive haemorrhage - binder early. |
| Septic Arthritis Triad | Hot swollen joint
Pain on movement Systemic upset |
Joint infection | Aspiration before antibiotics whenever possible. |
| SLE Activity Triad | Anti-dsDNA ↑
Complement ↓ CRP ± |
Active lupus | Helps differentiate flare from infection (use PCT). |
📌 Makindo master pearl: Triads are cognitive scaffolds, not diagnostic rules. Patients frequently present with partial or evolving triads - physiology, trajectory, and context always matter more than pattern recall.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery