
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
CADASIL
Related Subjects: |Neurological History taking |Causes of Stroke |Ischaemic Stroke |Hypertension |Small Vessel Disease |CADASIL |CARASIL
🧠 CADASIL (Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy) is the most common hereditary small vessel disease. It causes migraine, lacunar strokes, cognitive decline, psychiatric symptoms, and progressive neurological disability. Always ask about migraine and a family history of stroke/dementia in young stroke patients.
📌 Introduction
- CADASIL is a non-amyloid, non-arteriosclerotic microangiopathy of small cerebral arteries.
- Highly penetrant, usually presenting in mid-adulthood.
- Eventually leads to disability and dementia. Migraine with aura occurs in ~40%.
📊 Prevalence
- Estimated at 2–5 per 100,000 clinically diagnosed.
- Genetic database studies suggest NOTCH3 mutations may be as common as 3–4 per 1000.
💡 CADASIL is a “pure” monogenic form of cerebral small vessel disease (SVD), often with white matter strokes + microbleeds on MRI. Consider in any young patient with lacunar stroke + family history.
🧬 Aetiology
- Inheritance: Autosomal dominant, high penetrance. (Rarely, AR form = CARASIL).
- Gene: Mutated NOTCH3 on chromosome 19p13.1.
- Pathology: Accumulation of NOTCH3 protein around smooth muscle cells & pericytes, with Granular Osmiophilic Material (GOM) in vessel walls.
- GOM deposits also found in skin → explains systemic involvement.
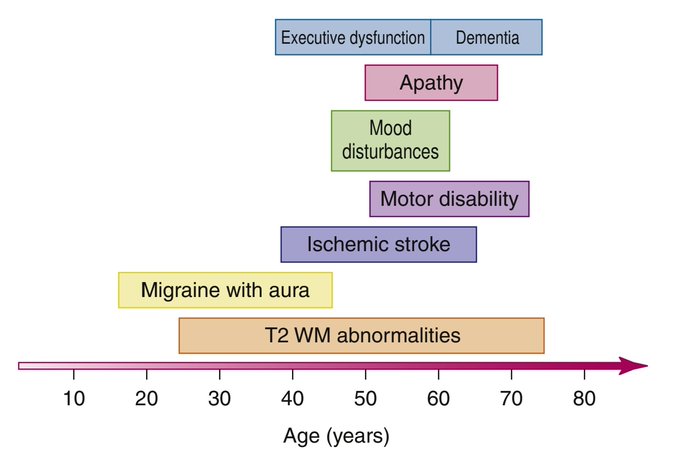
🩺 Clinical Aspects (The 5 “CADASIL pillars”)
- 1. Migraine with aura: Often <30 yrs onset, sometimes severe/complex with visual & sensory symptoms. Seen in ~40%.
- 2. Subcortical ischaemic events: Lacunar syndromes from 40s–50s, worsened by smoking, diabetes, hypertension.
- 3. Psychiatric features: Depression, anxiety, apathy, or bipolar-type illness.
- 4. Cognitive decline: From 40s, progressive → dementia by 60s. – Episodes of encephalopathy: transient confusion, reduced consciousness, seizures after migraine → recover in 1–2 weeks.
- 5. Progressive neurology: Gait apraxia, pseudobulbar palsy, incontinence. Less often seizures or parkinsonism.
🚩 Systemic clues: GOM deposits also found in skin and kidney → systemic involvement possible.
🧪 Investigations
- Bloods: Usually normal.
- CT head: Non-specific periventricular white matter change.
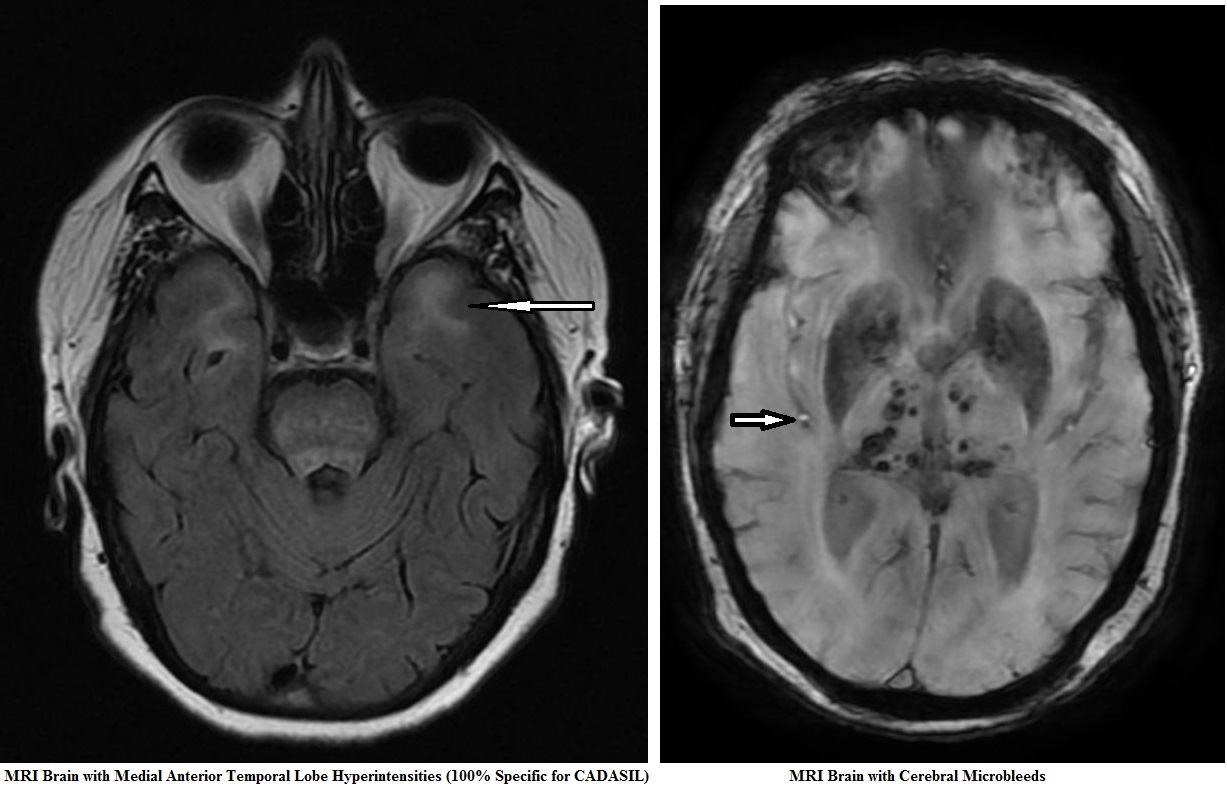
- MRI brain: Symmetrical white matter hyperintensities, especially in anterior temporal lobes & external capsule. – Microbleeds in ~50% (on GRE/T2*). – Progressive atrophy.
- Histology: Arterial wall eosinophilic deposits, smooth muscle apoptosis.
- Skin biopsy: NOTCH3 immunostaining (85–95% sensitive; 95–100% specific). GOM on EM = diagnostic.
- Genetic testing: Confirms NOTCH3 mutation. – Only do in classical phenotype (FHx + migraine with aura + SVD features).
💡 Imaging tip: – White matter changes in anterior temporal poles → Sensitivity 89%, Specificity 86%. – External capsule lesions → Sensitivity 93%, but lower specificity.
🔎 Differentials
- Sporadic small vessel disease (age-related, hypertension, diabetes).
- Multiple sclerosis (white matter lesions in young adults).
💊 Management
- No curative treatment. Course may be slowly progressive over decades.
- Risk factor control: No smoking 🚭, strict BP control, manage vascular risks.
- Unclear role: Antiplatelets/statins (only if coexistent atherosclerosis/vascular risk).
- Experimental: Some use L-arginine for migraine/fatigue → no strong evidence.
- Genetic counselling: Essential for affected families.
- Screening: Should be supported with counselling; prenatal screening role unclear.
🧩 CARASIL
CARASIL = Cerebral Autosomal Recessive Arteriopathy with Subcortical Infarcts and Leukoencephalopathy. – Caused by HTRA1 mutation. – Rarer, mainly in Japan/China. – Presents in 30s with stroke, cognitive decline, dementia, psychiatric change. – Associated with premature baldness, lumbar spondylosis, and back pain. – Imaging: diffuse WM disease + lacunar infarcts in basal ganglia/thalamus. – Pathology: arteriosclerosis, but no GOM.
📚 References
- NOTCH3 Mutations & CADASIL – Stroke, 2018
- Diagnostic Strategies in CADASIL – Neurology, 2002
- Chabriat H et al. CADASIL – Lancet Neurol, 2009
- CARASIL: from discovery to gene identification – J Stroke Cerebrovasc Dis, 2011
💡 Exam Pearl: Think of CADASIL in a 40–50 y/o with recurrent lacunar strokes + migraine aura + family history. MRI clue: anterior temporal pole + external capsule white matter hyperintensities.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery