
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Shoulder Anterior Dislocations
Related Subjects: |Shoulder Anterior Dislocations |Shoulder: Posterior Dislocation |Shoulder: Sterno-Clavicular Joint Dislocation
💪 Anterior Shoulder Dislocation - the most common type of shoulder dislocation (≈90–95%). Occurs when the humeral head is displaced anteriorly from the glenoid fossa. ⚠️ Always check for axillary nerve injury and associated fractures.
📌 Introduction
- Accounts for the majority of shoulder dislocations.
- Usually due to external rotation + abduction injury (e.g., sports, fall on outstretched hand).
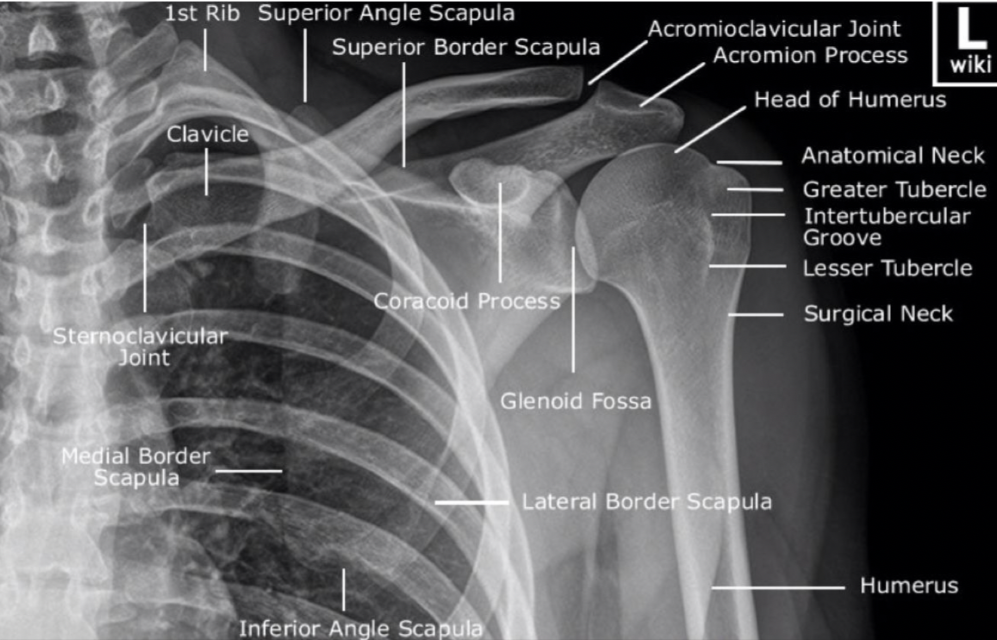
- Diagnosis: typically confirmed on anteroposterior (AP) shoulder X-ray.
🩻 Diagnosis & Initial Steps
- Establish IV access for analgesia/sedation.
- Give IV morphine or alternative for pain control.
- Request AP X-ray to confirm dislocation.
- Test and document axillary nerve function (badge-patch sensation over deltoid).
⚙️ Dislocation Management Algorithm
| Confirmed Dislocation ✅ | Alternative Diagnosis ❌ |
|---|---|
|
|
🛠️ Post-Reduction Care
- Repeat X-ray to confirm relocation.
- Reassess axillary nerve function.
- If reduction successful:
- Polysling + axillary pad.
- Adequate analgesia.
- Provide post-sedation discharge advice.
- Arrange fracture clinic (VFC) follow-up.
- If reduction unsuccessful:
- Maintain analgesia & polysling.
- Refer to on-call orthopaedics for further management.
🦴 Associated Fractures
Anterior shoulder dislocation is commonly associated with fracture of the greater tuberosity or surgical neck of the humerus.
- Undisplaced greater tuberosity fracture: Reduction may proceed as usual.
- Greater tuberosity displaced >1 cm: ❌ Do not attempt reduction - refer to orthopaedics for surgical management.
- Fracture neck of humerus: ❌ Do not attempt reduction - immediate orthopaedic referral.
🧾 Conclusion
- Anterior shoulder dislocation = common injury requiring urgent reduction & follow-up.
- Pain relief, safe sedation, and post-reduction monitoring are key for successful outcome.
- Always check for associated fractures & nerve injury - these alter management.
Cases - Anterior Shoulder Dislocation
- Case 1: A 22-year-old rugby player is tackled and falls with his arm outstretched. He presents with severe shoulder pain, arm held abducted and externally rotated, with a visible “squared off” contour. Distal pulses and sensation intact. X-ray confirms anteroinferior dislocation, no fracture. Management: IV analgesia, reduction performed under sedation using the Kocher manoeuvre, post-reduction X-ray confirms successful relocation. Sling and physiotherapy arranged. Outcome: Full recovery with physiotherapy; advised to avoid contact sport for 6 weeks. Counselling given about risk of recurrence, especially in young athletes.
- Case 2: A 68-year-old woman trips and falls onto her outstretched hand. She presents with severe shoulder pain, arm abducted and externally rotated, reduced sensation over the “regimental badge” area (axillary nerve). X-ray shows anterior dislocation with a small greater tuberosity fracture. Management: Procedural sedation and reduction achieved, but ongoing axillary nerve deficit noted. Post-reduction films confirm relocation. Orthopaedic team reviews fracture; conservative management chosen. Outcome: Shoulder mobilised in a sling for 3 weeks followed by physiotherapy. Nerve function partially recovers, but some persistent numbness remains.
Teaching Commentary 🧑⚕️
Anterior dislocation is the most common shoulder dislocation (>90%). Mechanism is typically fall on outstretched, abducted, externally rotated arm. Key signs are the squared-off contour and arm held away from the body. Always check for neurovascular compromise, especially the axillary nerve. Management is prompt analgesia, reduction, post-reduction X-ray, and physiotherapy. In young patients, recurrence is common; in older patients, associated fractures and nerve injury are more frequent. Tailor rehabilitation and follow-up accordingly.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery