Abdominal Aortic Aneurysm (AAA) ✅
Related Subjects:
Renal Colic
| Abdominal Aortic Aneurysm
| Acute Abdominal Pain
| Assessing Abdominal Pain
| Penetrating Abdominal Trauma
| Peripheral Arterial Disease (PAD)
|Abdominal Aortic Aneurysm (AAA)
| Carotid Endarterectomy
| Buerger's disease (Thromboangiitis obliterans )
| Leriche syndrome (aortoiliac occlusive disease)
| Vascular Surgery: Introduction
| Acute Limb Ischaemia
| Ankle-Brachial Pressure Index (ABPI) and Peripheral Vascular Disease
| Peripheral Arterial Disease (PAD)
| Abdominal Aortic Aneurysm (AAA)
| Carotid Endarterectomy
| Buerger's disease (Thromboangiitis obliterans)
| Leriche syndrome (aortoiliac occlusive disease)
|Acute Rhabdomyolysis
|Hyperkalaemia
|Acute Kidney Injury
🩸 Abdominal Aortic Aneurysm (AAA) – dilation of the abdominal aorta ≥3 cm. Surgical repair indicated when >5.5 cm, symptomatic, or rapidly enlarging. Mortality: ~6% elective repair vs up to 50% for emergency rupture ⚠️. Most common in >60 years, ♂ > ♀, strongly linked to smoking 🚬. Always consider AAA in elderly patients presenting with back or abdominal pain.
ℹ️ About AAA
- 📏 ≥50% increase in aortic diameter; abdominal aorta aneurysmal >3 cm.
- ⬇️ Most are infra-renal; may extend to iliac arteries.
- ⚠️ Surgery threshold: >5.5 cm, symptomatic, or rapid expansion.
- 📊 Morphology: fusiform (diffuse) vs saccular (focal outpouching).
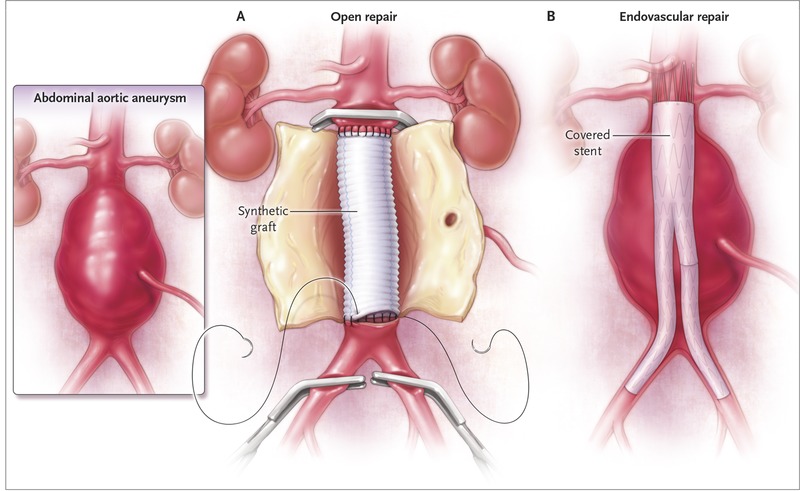 Diagram of an abdominal aortic aneurysm.
Diagram of an abdominal aortic aneurysm.
🧬 Aetiology & Pathophysiology
- 🦠 Chronic inflammation → elastin/collagen degradation → wall weakening.
- 🧬 Genetic predisposition: familial clustering, Marfan, Ehlers-Danlos syndromes.
- 💥 Larger aneurysm → higher wall tension → increased rupture risk.
- 🛑 Over-resuscitation may increase BP and worsen bleeding.
⚠️ Risk Factors
- 🚬 Smoking (strongest modifiable factor)
- 👴 Age >65, ♂ sex (5–10× risk)
- 🏋️ High BMI, tall stature, COPD
- 🧬 Connective tissue disorders (Marfan, EDS)
- 👨👩👦 Family history
- 💥 Rupture risk higher in ♀, large aneurysm (>5.5 cm), smokers, low FEV₁
🩺 Clinical Presentation
- 💥 Sudden, severe abdominal/back/flank pain ± groin radiation.
- 📉 Hypotension, shock.
- 🫀 Pulsatile abdominal mass (classic triad: pain + hypotension + mass in 25–50%).
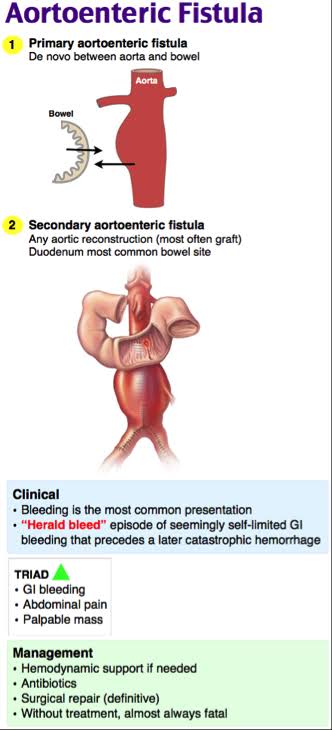
- 🛑 Rare: aorto-enteric fistula → GI bleed.
- 🦵 Distal emboli → limb ischaemia.
- 👴 Always exclude AAA in elderly males with acute back pain.
🎭 Differential Diagnoses of Ruptured AAA
| Differential |
Key Features / Clinical Clues |
Investigations |
| Appendicitis 🍎 |
RIF pain, gradual onset, anorexia 🤢, fever 🌡️, localised tenderness |
Abdominal USS / CT 🖼️, raised WBC / CRP 🧪 |
| Diverticulitis 💥 |
LLQ pain, altered bowel habits 💩, low-grade fever 🌡️ |
CT abdomen/pelvis 🖼️, inflammatory markers 🧪 |
| Aortic dissection 💔 |
Sudden severe tearing/ripping chest/back pain 🎯, syncope ⚡, pulse deficit 🩺 |
CT angiogram 🖼️, ECG 📈, CXR 🩻 |
| Renal colic / ureteric stone 🪨 |
Flank → groin pain 🌊, haematuria 🩸, restless patient 😖 |
Non-contrast CT KUB 🖼️, urinalysis 🧪, USS if CT unavailable |
| Perforated viscus 💥 |
Acute generalized abdominal pain 🎯, peritonism 🤕, rigid abdomen 🏋️♂️, shock ⚡ |
AXR 🩻, urgent CT abdomen 🖼️, labs for sepsis 🧪 |
| Myocardial infarction (STEMI/NSTEMI) ❤️🔥 |
Crushing central chest pain 🎯, radiation to jaw/arm 🦷🤚, dyspnoea 😤, diaphoresis 😓 |
12-lead ECG 📈, serial troponins 🧪, CXR 🩻 |
| Mesenteric ischaemia 🩸 |
Severe central abdominal pain out of proportion 🎯, vomiting 🤮, bloody stools 🩸 |
CT angiography 🖼️, lactate 🧪, metabolic bloods 🩸 |
| Gastrointestinal bleed (upper/lower) 🩸 |
Acute hypotension ⚡, melena/haematochezia 💩🩸, syncope 😵 |
FBC 🧪, crossmatch 🩸, endoscopy/colonoscopy 🖼️ |
| Ovarian torsion / ectopic pregnancy ⚠️ |
Lower abdominal pain 🤕, nausea/vomiting 🤢, amenorrhoea 🚫, vaginal bleeding 🩸 |
USS pelvis 🖼️, serum β-hCG 🧪, laparoscopy 🔪 if unstable |
🔎 Investigations
- 🩸 Bloods: FBC, U&E, LFTs, lactate, ABG, crossmatch.
- 🖼️ Imaging:
• Bedside USS: fast, ideal for unstable patients.
• CT angiogram: gold standard for stable patients, surgical planning.
⚠️ Do not delay transfer for CT if unstable.
- 📈 ECG, CXR supportive.
🚨 Emergency Management – Ruptured AAA
| 🚨 High Suspicion → Emergent Surgical Management |
|---|
- 🔎 Bedside USS or CT (if stable) to confirm diagnosis.
- 🔄 ABC: Airway, breathing, circulation. O₂ if hypoxic; permissive hypotension (SBP 90–120 mmHg).
- 💉 2× large-bore IV cannulas; crossmatch; prepare 6–10 units RBC, FFP, platelets.
- ⛔ Stop/reverse anticoagulants if possible.
- 📞 Alert anaesthetist + vascular surgeons; transfer to vascular centre within 30 min if required.
- ⚠️ Avoid unnecessary delays; knife-to-skin is priority in unstable patients.
|
🔪 Surgical Options
- Open Repair: Midline laparotomy, clamp aorta, insert Dacron/PTFE graft. High blood loss risk; ICU post-op.
- EVAR: Endovascular stent via femoral arteries; less invasive, lower immediate mortality, requires lifelong imaging follow-up for endoleaks.
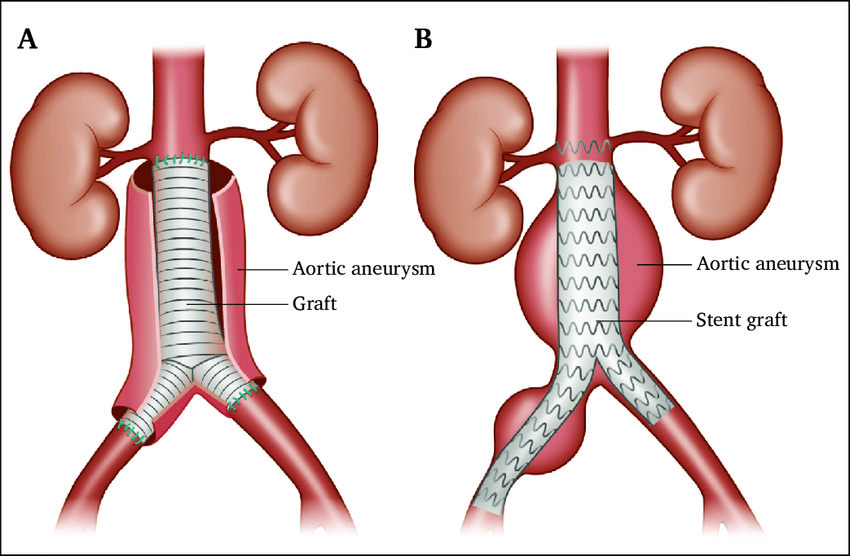 Open and endovascular AAA repair.
Open and endovascular AAA repair.
⚖️ Perioperative Considerations
- 📉 Pre-op: maintain SBP 90–120 mmHg.
- 💉 Intra-op: high transfusion requirement (RBC, FFP, platelets).
- 🏥 Post-op: ICU monitoring, watch for graft infection, AKI, multi-organ failure.
Case – Ruptured AAA
74M, smoker, hypertensive, sudden tearing abdominal/back pain, collapse, pallor, pulsatile mass, hypotensive/tachycardic. Bedside POCUS: large infrarenal AAA with free fluid. Management: ABCDE, 2 large-bore IVs, permissive hypotension (SBP ~80–90), activate major haemorrhage protocol, crossmatch blood, tranexamic acid per local policy, avoid unnecessary imaging, urgent vascular surgery consultation for definitive repair (EVAR if suitable; otherwise open). Post-op: monitor renal function, abdominal compartment syndrome, limb ischaemia, myocardial injury.
Case – Symptomatic (Unruptured) AAA
69M, known 5.6 cm infrarenal AAA, new constant deep abdominal/back pain, pulsatile mass, stable observations. Management: ABCDE, IV access, crossmatch, analgesia, cautious BP control, urgent CT angiography, early vascular surgery discussion for expedited repair (EVAR if suitable), NBM, monitor distal emboli (“blue toe”) and expansion. Education on smoking, hypertension, and UK repair thresholds.
📚 References
