
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Fibromuscular Dysplasia ✅
Related Subjects:Migraine |Basilar Migraine |Takayasu arteritis (pulseless disease) |Fibromuscular Dysplasia
⚠️ Fibromuscular Dysplasia (FMD) can cause four vascular changes: stenosis, aneurysm, dissection, or occlusion. Always consider in young stroke patients or those with refractory hypertension.
🧠 Introduction
- FMD is an idiopathic, non-inflammatory, and non-atherosclerotic disease of small- and medium-sized arteries.
- It leads to segmental arterial abnormalities affecting flow and structure.
- Most often affects the renal arteries and distal extracranial carotid arteries, but may involve multiple vascular beds.
- More common in young and middle-aged females (female:male ≈ 3:1).
- Accounts for a proportion of childhood strokes and young-onset renovascular hypertension.
🔍 Aetiology
- Found in ≈1% of carotid arteries at post-mortem studies.
- Segmental in nature: alternating areas of stenosis and dilation.
- Does not arise from atherosclerosis or vasculitis.
- Consider in ischaemic stroke or saccular aneurysms (with or without subarachnoid haemorrhage).
📑 Classification
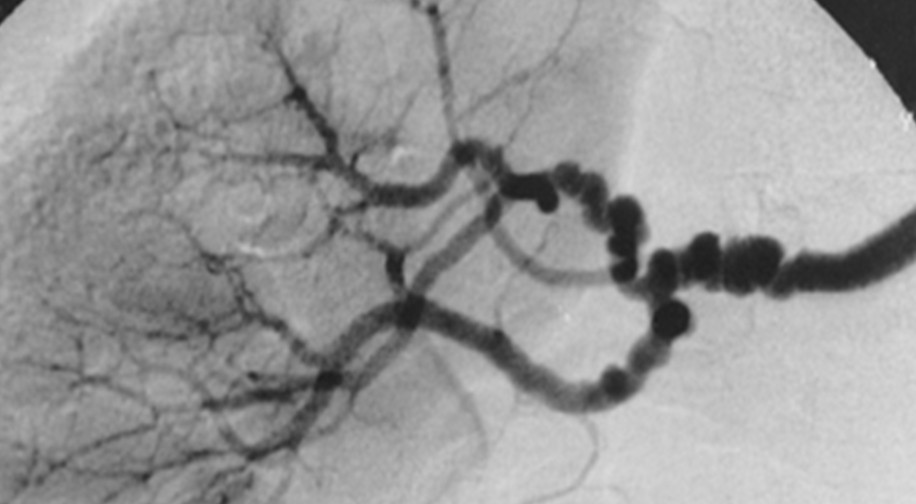
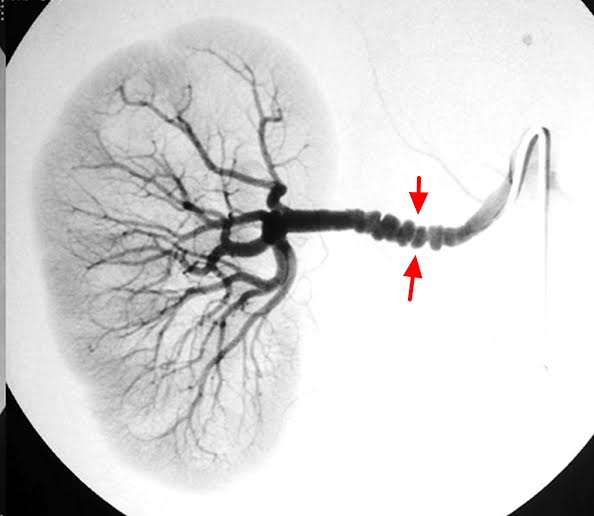
- 💢 Medial fibroplasia (≈80%) – Most common. Classic “string-of-beads” appearance on angiography. Multiple webs → stenosis with post-stenotic dilatation. Aneurysms frequent.
- 🧱 Intimal fibroplasia (≈10%) – Collagen deposition in intima. Appears as long tubular stenosis or concentric band-like narrowing.
- 👧 Perimedial fibroplasia (<10%) – Seen in young girls (5–15 years). Often presents with hypertension and renal dysfunction.
- 🔬 Medial hyperplasia (<1%) – Only confirmed pathologically.
- 🧩 Adventitial fibroplasia (<5%) – Seen on intravascular ultrasound (IVUS); angiography mimics intimal disease.
💡 Clinical Features
- Stroke or TIA due to carotid/vertebrobasilar infarction.
- Carotid/vertebral dissection causing headache, neck pain, or stroke.
- Renal artery stenosis → refractory hypertension.
- Carotid stenosis (with or without stroke).
- Spontaneous coronary artery dissection (SCAD) (link).
- Rare: pulmonary artery involvement.
- May present with subarachnoid haemorrhage from aneurysm rupture.
🧪 Investigations
- Bloods: FBC, U&E, creatinine (renal function).
- CT/MRI Brain: To detect infarction or SAH.
- Angiography (CTA / MRA / DSA): Shows stenosis with “string-of-beads”, dissections, or aneurysms.
- Histology (post-mortem/biopsy): Collagen deposition in intima/media, thinned media with beading.
- No validated genetic/ante-mortem biomarkers currently available.
🩺 Management
- 🚑 Ischaemic stroke: Follow standard stroke protocols (antiplatelets, BP control).
- 🩹 Dissections: Managed with antiplatelets short/long term.
- 🩻 Renal artery stenosis: May require percutaneous intervention or surgery.
- 💊 Hypertension: Treat with antihypertensive drugs.
- 🔁 Long-term follow-up with vascular imaging as disease can recur or progress.
📚 References & Further Reading
Diagnosis: Fibromuscular dysplasia. ⚡️ String-of-beads appearance in the renal artery is the classic clue. 📍 A nonatherosclerotic cause of renovascular hypertension in younger patients. 💡 Headache and tinnitus can fit associated carotid involvement
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery