
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Thalamic Haemorrhage
Related Subjects: |Subarachnoid Haemorrhage |Perimesencephalic Subarachnoid haemorrhage |Haemorrhagic stroke |Cerebellar Haemorrhage |Putaminal Haemorrhage |Thalamic Haemorrhage |ICH Classification and Severity Scores
🧠 Thalamic strokes can mimic sleepiness rather than coma. They arise from disruption of the thalamus, a key relay for sensory and motor pathways. Early recognition is crucial as prognosis depends on rapid imaging and management.
🔎 Introduction
Thalamic strokes involve an interruption of blood flow to the thalamus, a deep-seated structure acting as a relay centre for motor and sensory signals. They can be ischaemic or haemorrhagic and represent a small but important group of strokes. Clinical manifestations are varied - ranging from sensory loss and hemiparesis to visual field defects, memory impairment, and movement disorders.
🩸 Anatomy & Vascular Supply
- The thalamus is supplied by small penetrating arteries from the posterior cerebral artery (PCA) and posterior communicating artery (PComA).
- Paramedian arteries: from PCA (sometimes via a single artery of Percheron → bilateral thalamic infarcts).
- Tuberothalamic (polar) artery: from PComA → anterior thalamus.
- Thalamogeniculate arteries: from PCA → lateral thalamus.
- Posterior choroidal arteries: posterior thalamus & adjacent structures.
⚠️ Etiology
- Ischaemic infarction: small vessel disease (hypertension, diabetes), emboli, artery of Percheron occlusion.
- Haemorrhage: hypertensive bleeds, amyloid angiopathy, vascular malformations.
- Other: venous infarction (deep cerebral vein thrombosis), neoplasm, inflammatory lesions.
🧩 Clinical Features
- Sensory loss: contralateral hemianesthesia (all modalities).
- Motor weakness: contralateral hemiparesis from internal capsule involvement.
- Thalamic pain syndrome: chronic burning/aching pain weeks after stroke.
- Visual field defects: contralateral homonymous hemianopia/quadrantanopia.
- Oculomotor signs: vertical gaze palsy, light-near dissociation.
- Consciousness: drowsiness/coma in bilateral infarcts (esp. artery of Percheron).
- Cognitive & behavioural changes: memory impairment, apathy, disorientation.
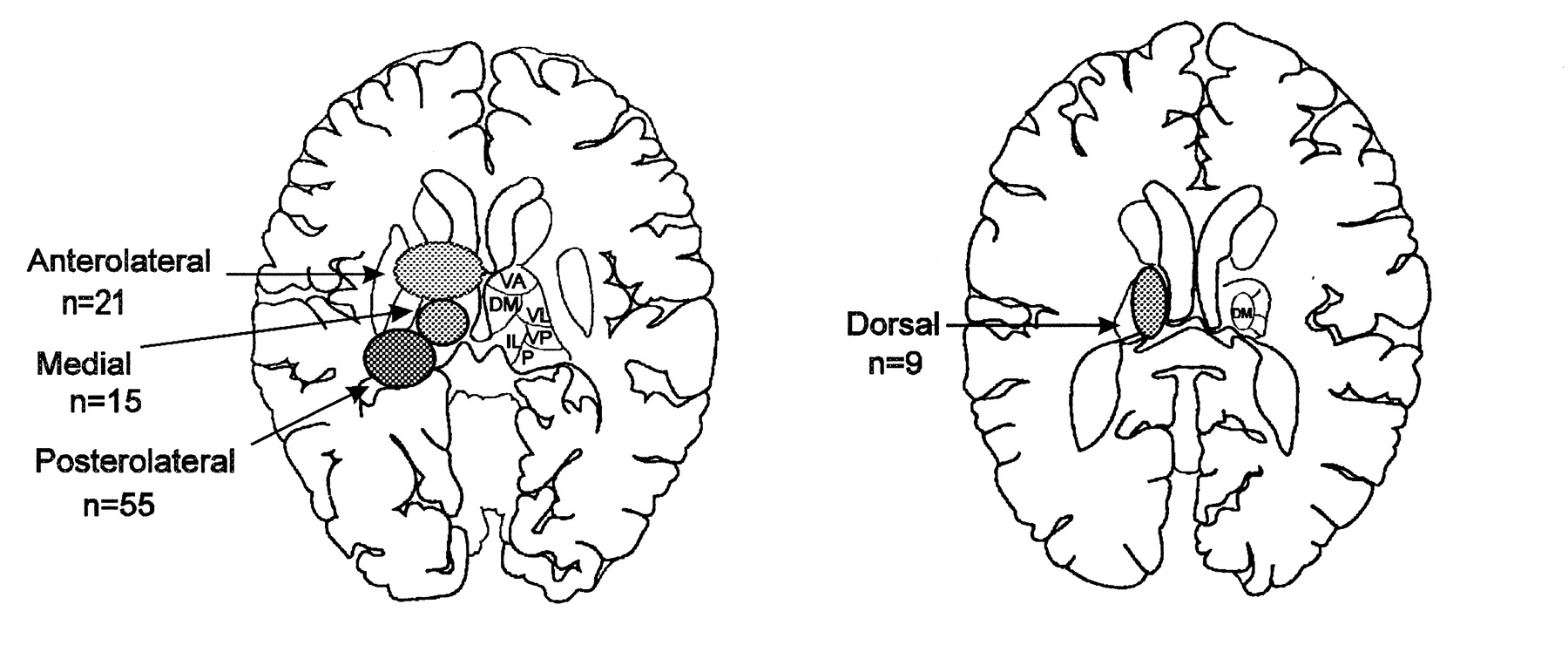
📊 Vascular Territories & Syndromes
| Artery | Clinical Syndrome |
|---|---|
| Paramedian (incl. artery of Percheron) | ⬇️ Consciousness, vertical gaze palsy, memory impairment |
| Tuberothalamic (polar) | Language disturbance, memory issues, apathy |
| Thalamogeniculate | Contralateral sensory loss, hemiparesis, movement disorders |
| Posterior choroidal | Visual field defects, ataxia, hemisensory loss |
🚨 Artery of Percheron infarct: Rare cause of sudden coma with bilateral thalamic and midbrain infarcts. Look for vertical gaze palsy + memory loss - a high-yield exam favourite!
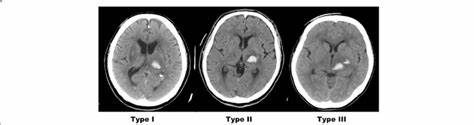
🖼️ Imaging
- CT head (non-contrast): first-line to exclude haemorrhage.
- MRI DWI: best for small acute infarcts.
- CTA/MRA: shows PCA/PComA anatomy, can detect artery of Percheron occlusion.
- DSA: gold standard if vascular malformation suspected.
🧪 Investigations
- Bloods: FBC, U&E, glucose, lipids, clotting.
- ECG ± Holter: atrial fibrillation, arrhythmias.
- Echocardiogram: cardiac embolic source.
- Risk factors: BP monitoring, HbA1c.
🚑 Acute Management
- Ischaemic: IV thrombolysis ≤4.5h (if eligible), mechanical thrombectomy up to 6h (≤24h in selected cases), start antiplatelets once haemorrhage excluded.
- Haemorrhagic: strict BP control, neuro ICU, manage ICP, neurosurgical opinion.
🔄 Secondary Prevention
- Antiplatelets (aspirin, clopidogrel) or anticoagulation if cardioembolic.
- Statins (LDL reduction + plaque stabilisation).
- Risk factor control: BP, diabetes, smoking cessation, exercise.
🧑🦽 Rehabilitation
- Physio: motor recovery, gait training.
- OT: daily living adaptations.
- SLT: dysarthria, dysphagia.
- Pain team: for thalamic pain syndrome (antidepressants, anticonvulsants).
- Psychological support for depression, fatigue, cognitive issues.
📈 Prognosis
- Many recover function, but persistent sensory loss and pain are common.
- Haemorrhagic strokes carry higher mortality.
- Bilateral thalamic infarcts have poor outcomes if coma persists.
📚 References
- Schmahmann JD. Vascular syndromes of the thalamus. Stroke. 2003.
- Adams HP Jr et al. Guidelines for early management of adults with ischaemic stroke. Stroke. 2007.
- Guenego A et al. Artery of Percheron infarct. Neuroradiology. 2015.
🖼️ Images
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery