
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Heart Block
Related Subjects: |Resus:Bradycardia |Resus:Tachycardia | Syncope | Transient Loss of Consciousness | Aortic Stenosis | Breast Cancer
⚡ Severe Bradycardia - Management (UK ALS)
| Step | What you do (OSCE/ALS wording) | Key notes / triggers |
|---|---|---|
| 1) Recognise severity | 🔍 Confirm bradycardia on monitor/ECG, check pulse + BP, assess symptoms. | 🚨 Treat as unstable if any adverse features: shock, syncope, MI/ischaemia, acute HF. |
| 2) Call for help + monitor | 📞 Call resus team/senior help, attach defib/pacing pads, continuous ECG + SpO2 + NIBP. | Have pacing ready early if high-grade AV block suspected. |
| 3) ABCDE + access | 🫁 ABCDE, oxygen only if hypoxic, 2 IV cannulas, take bloods (U&E, Mg, glucose, VBG/ABG if unwell). | Look for reversible causes: drug toxicity (β-blocker, digoxin, CCB), hyperkalaemia, hypoxia, MI. |
| 4) ECG | 📈 Get a 12-lead ECG (rhythm + PR/QRS, ischaemia, AV block). | High-risk ECG: Mobitz II, complete heart block, broad QRS escape, long pauses. |
| 5) First-line drug | 💉 Atropine 500 micrograms IV; repeat as needed to max 3 mg. | Less effective in infra-His block; avoid/seek specialist advice in transplanted heart. |
| 6) If no response / unstable | ⚡ Start transcutaneous pacing (with analgesia/sedation support) while preparing for definitive pacing. | Don’t delay pacing if high-grade AV block or recurrent syncope/shock. |
| 7) If pacing not available / bridging | 💧 Start an infusion per local protocol: adrenaline 2–10 micrograms/min OR isoprenaline 5 micrograms/min OR dopamine. | Use as a bridge to pacing; monitor for tachyarrhythmia/ischaemia. |
| 8) Definitive management | 🧑⚕️ Arrange temporary transvenous pacing ± permanent pacemaker; treat cause (MI pathway, stop culprit drugs, treat hyperkalaemia). | Complete heart block / Mobitz II usually needs pacing; document decisions + escalation. |
⚡ Heart block (AV block) describes delayed or failed conduction from atria → ventricles. A slow heart rate - cunt QRS complexes can lead to low blood pressure and even shock. This may need emergent treatment. Exam focus: recognise the ECG pattern, assess stability, correct reversible causes, and escalate early for pacing when needed.
🧠 What “heart block” actually means
- 🔌 The AV node–His–Purkinje system is the only normal electrical bridge from atria to ventricles.
- ⛔ “Block” can be partial (delay or intermittent failure) or complete (no impulses conducted).
- 🫀 When ventricles don’t receive atrial impulses, they rely on an escape rhythm:
- ⬆️ Higher (junctional) escape → faster rate, usually narrow QRS.
- ⬇️ Lower (ventricular) escape → slower rate, usually wide QRS.
📊 First vs Second vs Third Degree AV Block (high-yield comparison)
| Type | ECG hallmark | What you do (exam / ward) |
|---|---|---|
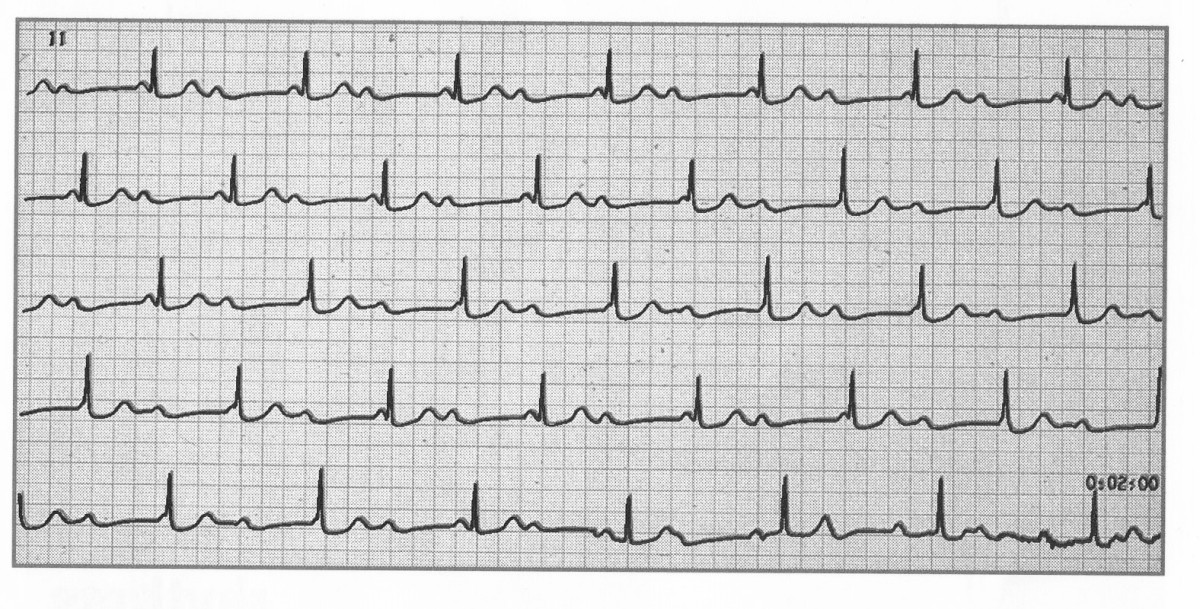
| 1️⃣ First-degree AV block | PR > 200 ms, constant; every P followed by QRS | Usually observe ✅; review AV-nodal drugs; check U&E (K+/Mg), TFTs; treat underlying cause |
| 2️⃣a 🔁 Mobitz I (Wenckebach) | Progressive PR prolongation → then dropped QRS | If stable: remove triggers/hold AV-nodal drugs, observe; if symptomatic/unstable: manage bradycardia + senior/cardiology review |
| 2️⃣b ⚠️ Mobitz II | Fixed PR with intermittent dropped QRS (often wide QRS) | High-risk 🚨: urgent cardiology; prepare for pacing (often pacing-likely even if transient); treat instability per ALS (pacing preferred) |
| 3️⃣ 🚑 Third-degree (complete) heart block | AV dissociation: P waves and QRS regular but independent; escape rhythm (narrow if high, wide if low) | Time-critical: ABCDE, stop causative drugs, treat reversible causes; atropine may help if nodal; isoprenaline/temporary pacing if needed → usually permanent pacemaker |
🚨 Red flags that should make you escalate immediately
- 🧠 Syncope, recurrent presyncope, confusion
- 🫀 Hypotension, shock, chest pain, acute heart failure, ischaemic ECG changes
- 🧍 Very slow ventricular rate (especially < 40 bpm) or broad-complex escape rhythm
- ⚡ Mobitz II, high-grade AV block (multiple consecutive dropped beats), or complete heart block
🧩 Causes of AV block (exam-friendly table)
| Category | Examples | Clues |
|---|---|---|
| ❤️ Ischaemia / MI | Inferior MI (RCA → AV nodal branch), anterior MI (His–Purkinje damage) | Inferior MI block may respond to atropine and can be transient; anterior MI block is often extensive disease and higher risk. |
| 💊 Drugs | β-blockers, verapamil/diltiazem, digoxin, amiodarone (and other antiarrhythmics) | Recent dose change, renal impairment (digoxin), bradycardia + hypotension. |
| 🧓 Degenerative conduction disease | Fibrosis/sclerosis of the conduction system (age-related) | Older patient, bundle branch block, progressive conduction delay. |
| 🦠 Infective / inflammatory | Myocarditis, endocarditis (peri-annular abscess), Lyme disease, diphtheria | Fever, raised inflammatory markers, new murmur, travel/tick exposure. |
| 🧬 Infiltrative / metabolic | Sarcoid, amyloid, haemochromatosis; hyperkalaemia; hypothyroidism | Systemic features; abnormal K+ / thyroid; unexplained conduction disease. |
| 🛠️ Post-procedure | TAVI, valve surgery, septal myectomy, ablation | New conduction delay after intervention. |
🔎 Investigations (what to send in real life + OSCE)
- 📈 12-lead ECG + rhythm strip (confirm type of block; look for ischaemia).
- 🩺 Obs + perfusion: BP, mental status, cap refill; signs of heart failure.
- 🧪 Bloods: U&E (K+), Mg, Ca, glucose, FBC, CRP, TFTs; troponin if ACS suspected; digoxin level if relevant.
- 🖥️ Echocardiography if structural disease/MI suspected or ongoing instability.
- 🧷 Consider continuous monitoring / telemetry and cardiology review for unexplained or high-grade block.
⚡ Acute management of bradycardia due to AV block (UK ALS-style)
🚑 If unstable: treat as a peri-arrest bradycardia. Start with ABCDE + attach monitoring, then correct reversible causes while preparing for pacing.
| Step | What you do | Why |
|---|---|---|
| 1️⃣ Call for help | 📞 Senior + cardiology; if peri-arrest, resus team/ALS response. | High-grade AV block can deteriorate rapidly. |
| 2️⃣ Stabilise | 🫁 Oxygen if hypoxic, IV access, fluids if shocked, treat pain, correct electrolytes. | Improve perfusion while definitive therapy is arranged. |
| 3️⃣ Atropine (if appropriate) | 💉 Atropine 500 micrograms IV, repeat to a maximum of 3 mg if needed. | May improve AV nodal block (often helpful in inferior MI / nodal disease). |
| 4️⃣ If atropine fails / high-risk block | ⚡ Prepare transcutaneous pacing early; consider isoprenaline infusion as a bridge if pacing not immediately available (specialist / local protocol). | In infranodal block, atropine may be ineffective; pacing prevents collapse. |
| 5️⃣ Definitive treatment | 🧷 Temporary pacing (wire) if needed → usually permanent pacemaker for persistent high-grade/complete AV block. | Prevents recurrence and improves long-term safety. |
🧠 Teaching pearls (sounds clever in vivas)
- 🧬 Nodal vs infranodal block: nodal block is more likely to respond to atropine and has a narrow QRS; infranodal block is more dangerous and often needs pacing.
- 🫀 Why syncope happens: slow escape rhythms reduce cardiac output → cerebral hypoperfusion (Stokes–Adams attacks).
- 🧯 Reversible causes matter: hyperkalaemia, AV nodal drugs, and ischaemia are the “big three” to look for quickly.
⛔ Complete (Third-degree) Heart Block - exam-ready
🚨 Complete heart block can be a medical emergency requiring atropine and pacing. It is defined by complete failure of conduction between atria and ventricles, so the ventricles rely on an escape rhythm.
ℹ️ About
- 🔌 There is a complete failure of communication between atria and ventricles.
- 💓 Atria depolarise regularly (P waves), but do not stimulate the ventricles.
- 🫀 Ventricles beat at an intrinsic escape rate, often ~30–40 bpm if ventricular, faster if junctional.
- 📏 The higher the escape rhythm (closer to AV node), the faster the rate and the narrower the QRS.
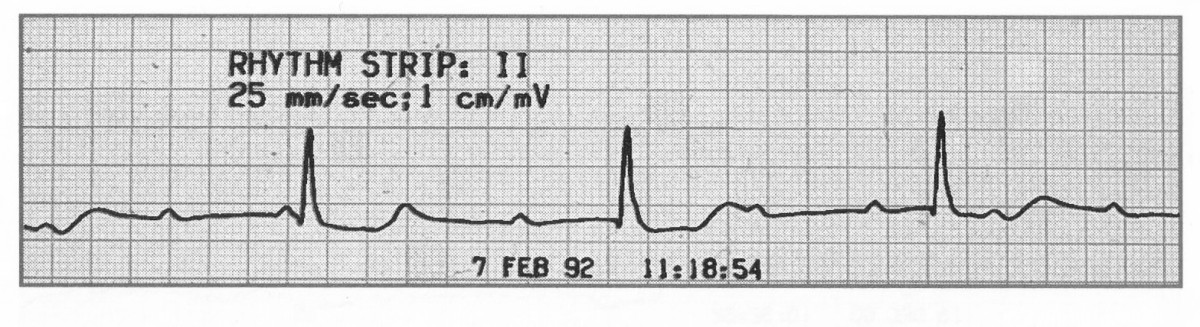
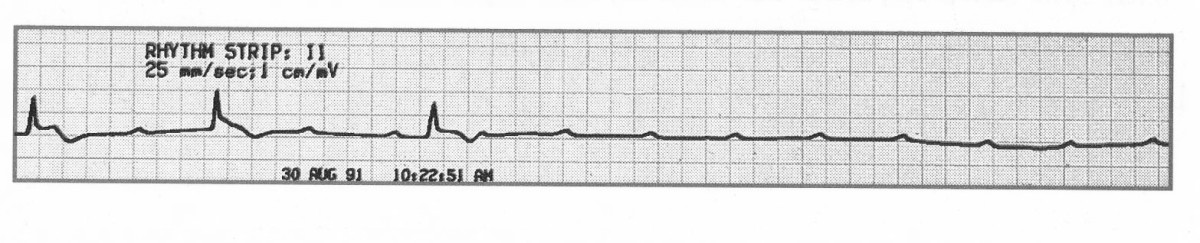
📈 ECG features
- Atrial rate: typically 60–100/min (sinus), independent of the ventricular rhythm (“dissociation”).
- Ventricular rate: depends on escape focus:
- 🐢 Ventricular escape typically ~20–40/min (often wide QRS).
- ⚡ Junctional escape typically ~40–60/min (often narrow QRS).
- Rhythm: atrial and ventricular rhythms are each regular but independent.
- PR interval: no fixed PR relationship (by definition).
- P waves: usually normal morphology (unless AF/atrial flutter etc.).
- QRS: narrow suggests higher escape; wide suggests lower (infranodal) escape.
- 🧠 Note: If the atrial rhythm is atrial fibrillation, there are no P waves-you’ll see a slow regular escape rhythm with AV dissociation.
🧩 Causes
- ❤️ Inferior MI (RCA involvement affecting AV nodal blood supply) - can be transient.
- 🧱 Anterior MI - suggests extensive myocardial/conduction system damage; often more unstable.
- 💊 Medications: β-blockers, digoxin, rate-limiting calcium-channel blockers (verapamil/diltiazem), and some antiarrhythmics.
- 🧓 Degenerative fibrosis/sclerosis of conduction tissue (older adults).
- 🦠 Myocarditis, endocarditis (incl. peri-annular abscess), post-surgery, rheumatic fever.
- 🪲 Lyme disease, diphtheria (rare in UK but classic exam causes).
🩺 Clinical features
- 🚑 Acute: symptomatic bradycardia, low BP, shock, syncope (Stokes–Adams), acute heart failure.
- 🧍 Chronic: reduced exercise tolerance, fatigue, dizziness/presyncope.
- 🌊 JVP: cannon “a” waves can occur due to atrial contraction against a closed tricuspid valve.
🔎 Investigations
- 📈 ECG (diagnostic) + continuous monitoring.
- 🧪 U&E (K+), Mg/Ca, TFTs, glucose; troponin if ACS suspected; drug levels where relevant (e.g., digoxin).
- 🖥️ Echo if structural disease/MI suspected or ongoing instability.
💊 Management
- 🛟 ABCDE and resuscitation as needed; treat shock/ACS in parallel.
- 💉 Consider atropine, isoprenaline infusion (bridge), and temporary pacing (transcutaneous → transvenous) depending on stability and ECG features.
- 🧯 Treat reversible causes: stop AV nodal drugs, correct hyperkalaemia, manage MI/myocarditis/infection.
- 🧷 Most patients with persistent complete heart block will require a permanent pacemaker after specialist assessment.
📚 References (UK + core)
- Resuscitation Council UK. Concise adult bradyarrhythmia guidance (includes atropine dosing and escalation to pacing).
- British Heart Rhythm Society (BHRS). Standards for implantation and follow-up of cardiac rhythm management devices in adults (2024).
- ESC Guidelines on cardiac pacing and cardiac resynchronization therapy (2021).
- ACC/AHA/HRS Guideline on the evaluation and management of bradycardia and cardiac conduction delay (2018).
- BMJ Best Practice. Atrioventricular block.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery