
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Clinical Appearance Collections
🟤 Diffuse hyperpigmentation (palmar creases, scars, mucosa) due to ↑ ACTH → primary adrenal failure.
Actinomyces
🦷 Chronic indurated cervicofacial infection with sinus tracts and “sulphur granules”.

Achenbach Syndrome
🩸 Sudden painful blue finger due to spontaneous venous bleeding - benign and self-limiting.

Acanthosis
⚫ Velvety hyperpigmentation of flexures - insulin resistance; sudden onset → consider malignancy.

Acne
🧴 Comedones, papules, pustules - androgen-driven pilosebaceous inflammation.

Acne Rosacea
🌹 Facial flushing, telangiectasia, papules; no comedones.

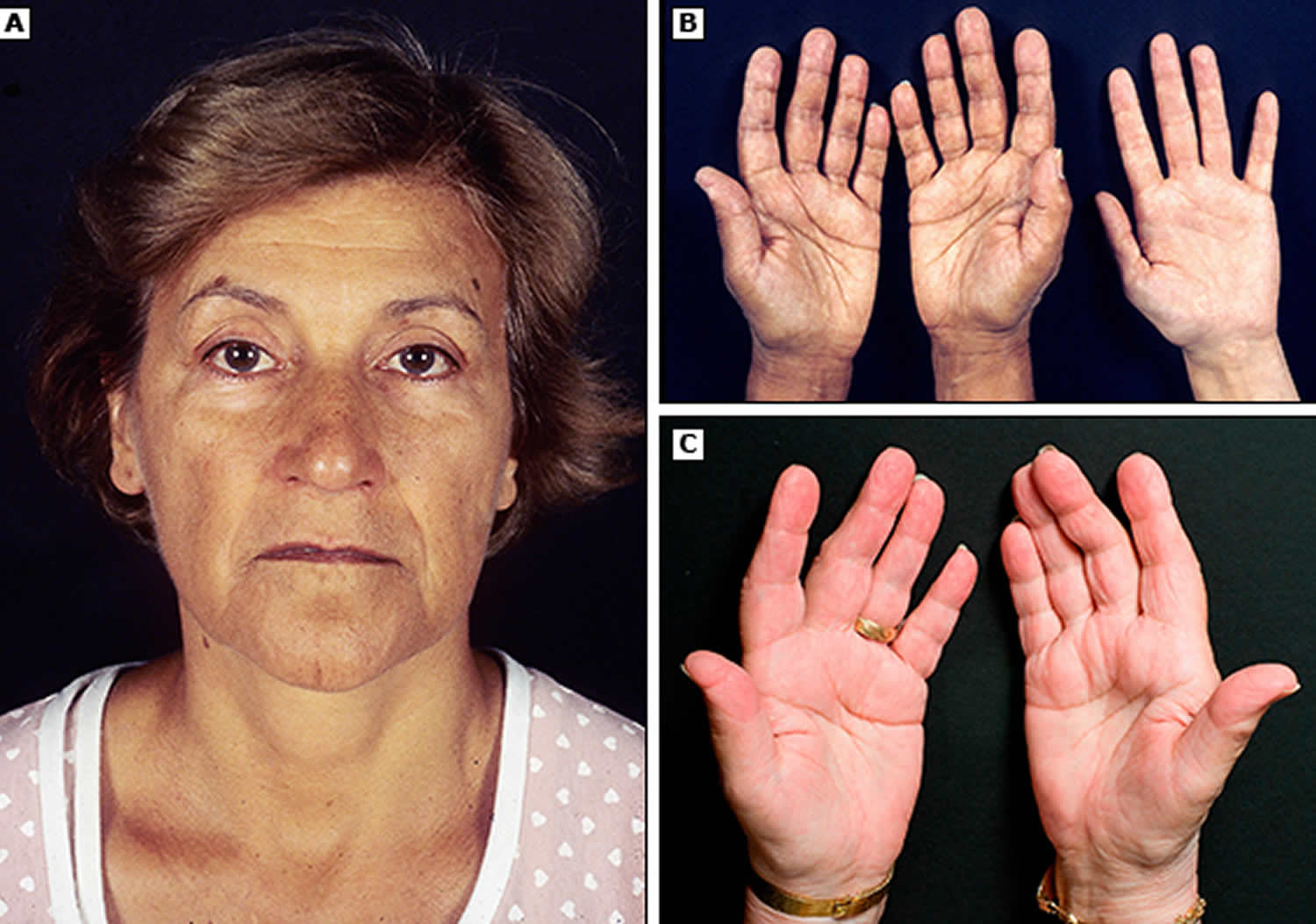
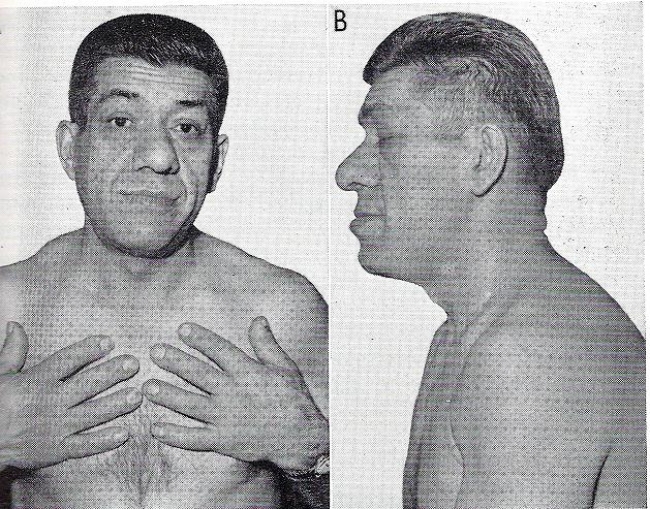
Acromegaly
🦴 Enlarged hands, jaw, coarse features - excess GH, usually pituitary adenoma.
Angioneurotic oedema
💥 Sudden non-pitting swelling of lips/tongue; ACE-I causes bradykinin-mediated disease.

Ameloblastoma
🦷 Slow-growing jaw tumour - locally aggressive, classically “soap-bubble” appearance.

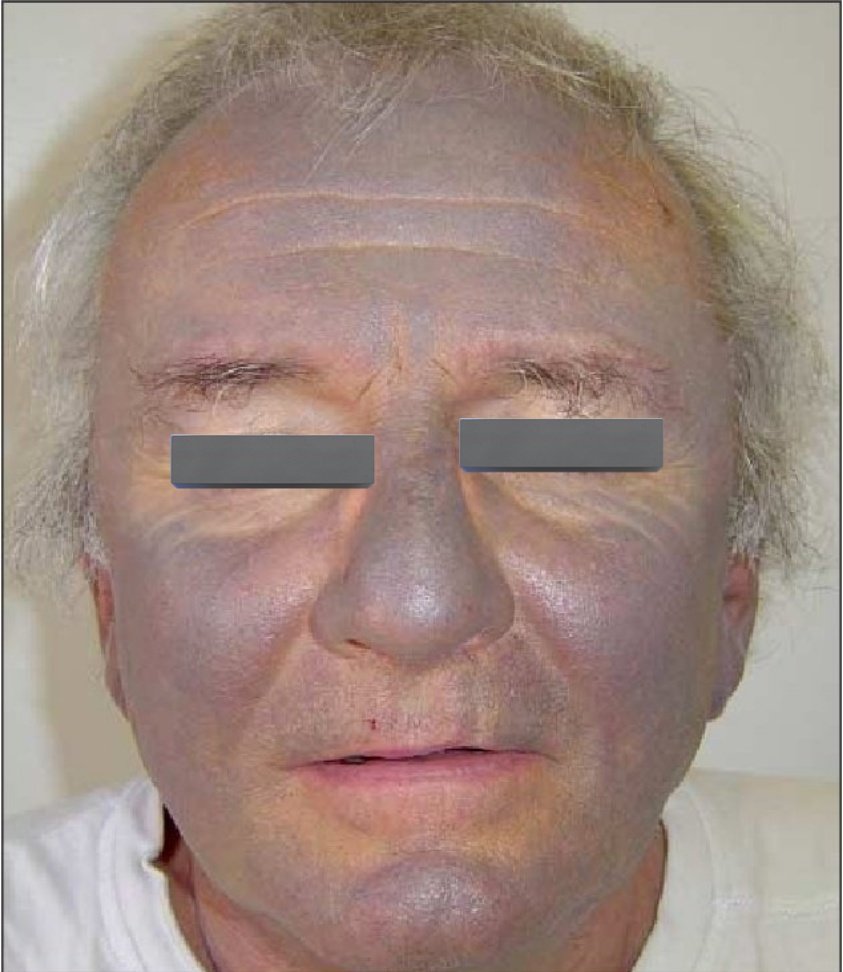
Amiodarone
🔵 Blue-grey skin pigmentation and photosensitivity with long-term use.
Down syndrome
🧬 Trisomy 21 - upslanting palpebral fissures, hypotonia, single palmar crease.

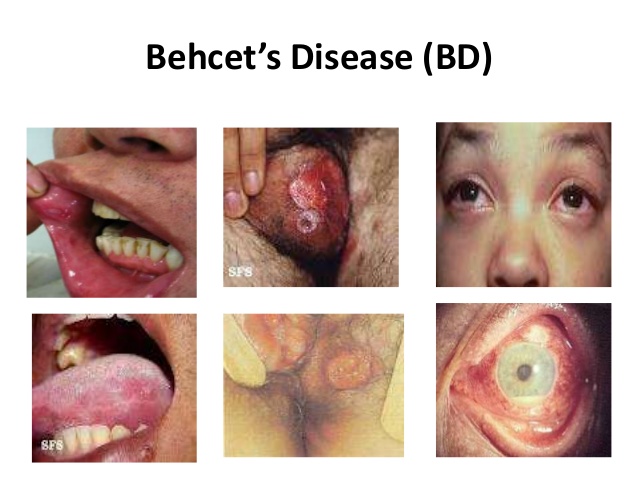
Behcet syndrome
🔥 Recurrent oral and genital ulcers with uveitis - systemic vasculitis.
Neurofibromatosis
☕ Café-au-lait spots, neurofibromas; NF1 → optic glioma, NF2 → bilateral acoustic neuromas.




Monkey pox
🦠 Umbilicated vesiculopustular lesions with systemic symptoms.

Myotonic dystrophy
✋ Delayed muscle relaxation, frontal balding, cataracts.

Hurler syndrome
🧬 Gargoyle facies, corneal clouding, hepatosplenomegaly - MPS I.

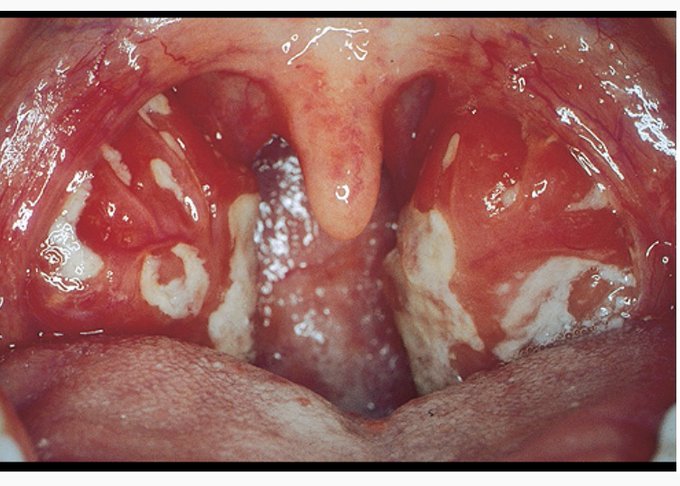
EBV / Mononucleosis
💋 Fever, lymphadenopathy, exudative tonsillitis ± splenomegaly.
Penicillin + EBV rash
💊 Generalised maculopapular rash - not a true penicillin allergy.

Pressure Ulcers
🛏️ Non-blanching skin damage over pressure points.

Hereditary Haemorrhagic Telangiectasia
🩸 Telangiectasia + recurrent epistaxis → think AVMs.

Cutaneous Anthrax
⚫ Painless black eschar with surrounding oedema.

Lyme disease
🎯 Erythema migrans “bull’s-eye” rash.

Molluscum contagiosum
⚪ Umbilicated pearly papules - poxvirus.

Clubbing
🫁 Bulbous fingertips - chronic hypoxia or malignancy.

Cushing's syndrome
🌙 Moon face, truncal obesity, purple striae - cortisol excess.

Thyrotoxicosis
🔥 Key clinical clues: weight loss, heat intolerance, tremor, anxiety, diarrhoea, palpitations.
❤️ Exam: tachycardia/AF, warm sweaty skin, fine tremor, hyperreflexia; goitre ± bruit; Graves’ signs (lid lag, ophthalmopathy).
🧪 Tests: ↓TSH with ↑free T4/T3; check TSH receptor antibodies; consider thyroid uptake scan if unclear; baseline FBC/LFTs before carbimazole.
⚠️ Red flags: thyroid storm (fever, delirium, severe tachycardia), AF with fast rate, heart failure in older adults (often “apathetic hyperthyroidism”).
💊 Management: beta-blocker for symptoms; antithyroid drugs (carbimazole/PTU), radioiodine or surgery depending on cause and relapse risk.

Wilson Disease – Kayser–Fleischer Ring
👁️🟤 What you’re seeing: copper deposition in Descemet’s membrane causing a brown-green corneal ring.
🧠 Think Wilson if: young person with liver disease + neuropsychiatric symptoms (tremor, dystonia, dysarthria, personality change).
🧪 Tests: low caeruloplasmin, ↑24h urinary copper, liver copper on biopsy; slit-lamp exam confirms subtle rings.
⚠️ Pearl: haemolysis can occur (Coombs-negative) due to copper toxicity.
💊 Treatment: chelation (penicillamine or trientine) + zinc; transplant if fulminant liver failure.

Cutaneous Larva Migrans on Leg
🐛 Classic appearance: intensely itchy, serpiginous “creeping eruption” track advancing daily.
🏖️ Cause: hookworm larvae (often from dog/cat faeces in warm sandy soil) migrating within superficial skin layers.
🩺 Symptoms: marked pruritus; secondary bacterial infection from scratching is common.
🧪 Diagnosis: usually clinical; blood eosinophilia is variable and not required.
💊 Treatment: ivermectin (often single dose) or albendazole; antihistamines/topical steroids for itch; advise footwear and avoidance of contaminated sand.

Addison's disease
🟤 Diffuse hyperpigmentation (palmar creases, scars, mucosa) due to ↑ ACTH → primary adrenal failure.
Actinomyces
🦷 Chronic indurated cervicofacial infection with sinus tracts and “sulphur granules”.
Achenbach Syndrome
🩸 Sudden painful blue finger due to spontaneous venous bleeding - benign and self-limiting.
Acanthosis
⚫ Velvety hyperpigmentation of flexures - insulin resistance; sudden onset → consider malignancy.
Acne
🧴 Comedones, papules, pustules - androgen-driven pilosebaceous inflammation.
Acne Rosacea
🌹 Facial flushing, telangiectasia, papules; no comedones.
Acromegaly
🦴 Enlarged hands, jaw, coarse features - excess GH, usually pituitary adenoma.
Angioneurotic oedema
💥 Sudden non-pitting swelling of lips/tongue; ACE-I causes bradykinin-mediated disease.
Ameloblastoma
🦷 Slow-growing jaw tumour - locally aggressive, classically “soap-bubble” appearance.
Amiodarone
🔵 Blue-grey skin pigmentation and photosensitivity with long-term use.
Down syndrome
🧬 Trisomy 21 - upslanting palpebral fissures, hypotonia, single palmar crease.
Behcet syndrome
🔥 Recurrent oral and genital ulcers with uveitis - systemic vasculitis.
Neurofibromatosis
☕ Café-au-lait spots, neurofibromas; NF1 → optic glioma, NF2 → bilateral acoustic neuromas.
Monkey pox
🦠 Umbilicated vesiculopustular lesions with systemic symptoms.
Myotonic dystrophy
✋ Delayed muscle relaxation, frontal balding, cataracts.
Hurler syndrome
🧬 Gargoyle facies, corneal clouding, hepatosplenomegaly - MPS I.
EBV / Mononucleosis
💋 Fever, lymphadenopathy, exudative tonsillitis ± splenomegaly.
Penicillin + EBV rash
💊 Generalised maculopapular rash - not a true penicillin allergy.
Pressure Ulcers
🛏️ Non-blanching skin damage over pressure points.
Hereditary Haemorrhagic Telangiectasia
🩸 Telangiectasia + recurrent epistaxis → think AVMs.
Cutaneous Anthrax
⚫ Painless black eschar with surrounding oedema.
Lyme disease
🎯 Erythema migrans “bull’s-eye” rash.
Molluscum contagiosum
⚪ Umbilicated pearly papules - poxvirus.
Clubbing
🫁 Bulbous fingertips - chronic hypoxia or malignancy.
Cushing's syndrome
🌙 Moon face, truncal obesity, purple striae - cortisol excess.
Thyrotoxicosis
🔥 Key clinical clues: weight loss, heat intolerance, tremor, anxiety, diarrhoea, palpitations.
❤️ Exam: tachycardia/AF, warm sweaty skin, fine tremor, hyperreflexia; goitre ± bruit; Graves’ signs (lid lag, ophthalmopathy).
🧪 Tests: ↓TSH with ↑free T4/T3; check TSH receptor antibodies; consider thyroid uptake scan if unclear; baseline FBC/LFTs before carbimazole.
⚠️ Red flags: thyroid storm (fever, delirium, severe tachycardia), AF with fast rate, heart failure in older adults (often “apathetic hyperthyroidism”).
💊 Management: beta-blocker for symptoms; antithyroid drugs (carbimazole/PTU), radioiodine or surgery depending on cause and relapse risk.
Wilson Disease – Kayser–Fleischer Ring
👁️🟤 What you’re seeing: copper deposition in Descemet’s membrane causing a brown-green corneal ring.
🧠 Think Wilson if: young person with liver disease + neuropsychiatric symptoms (tremor, dystonia, dysarthria, personality change).
🧪 Tests: low caeruloplasmin, ↑24h urinary copper, liver copper on biopsy; slit-lamp exam confirms subtle rings.
⚠️ Pearl: haemolysis can occur (Coombs-negative) due to copper toxicity.
💊 Treatment: chelation (penicillamine or trientine) + zinc; transplant if fulminant liver failure.
Cutaneous Larva Migrans on Leg
🐛 Classic appearance: intensely itchy, serpiginous “creeping eruption” track advancing daily.
🏖️ Cause: hookworm larvae (often from dog/cat faeces in warm sandy soil) migrating within superficial skin layers.
🩺 Symptoms: marked pruritus; secondary bacterial infection from scratching is common.
🧪 Diagnosis: usually clinical; blood eosinophilia is variable and not required.
💊 Treatment: ivermectin (often single dose) or albendazole; antihistamines/topical steroids for itch; advise footwear and avoidance of contaminated sand.
Gorlin’s sign 👅

- Definition: ability to touch the tip of the nose with the tongue.
- Meaning: a supportive clue to generalised hypermobility / connective tissue laxity (e.g., hypermobility spectrum/EDS), but not diagnostic.
- Next step: assess Beighton score + symptoms (sprains/dislocations, chronic pain) + skin features + family history.
Urticaria

| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery